
Radical Hysterectomy with Bilateral Salpingo-Oophorectomy
What is a radical hysterectomy with bilateral salpingo‑oophorectomy?
A radical hysterectomy with bilateral salpingo-oophorectomy is a surgical procedure commonly performed in gynecology to treat various conditions, including certain gynecological cancers and severe cases of endometriosis.
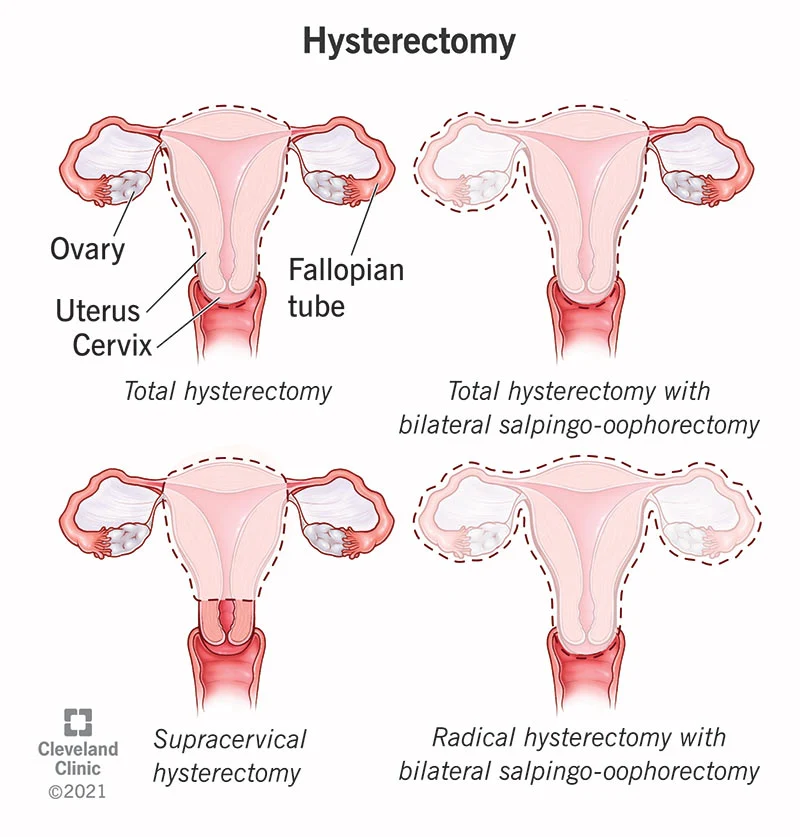
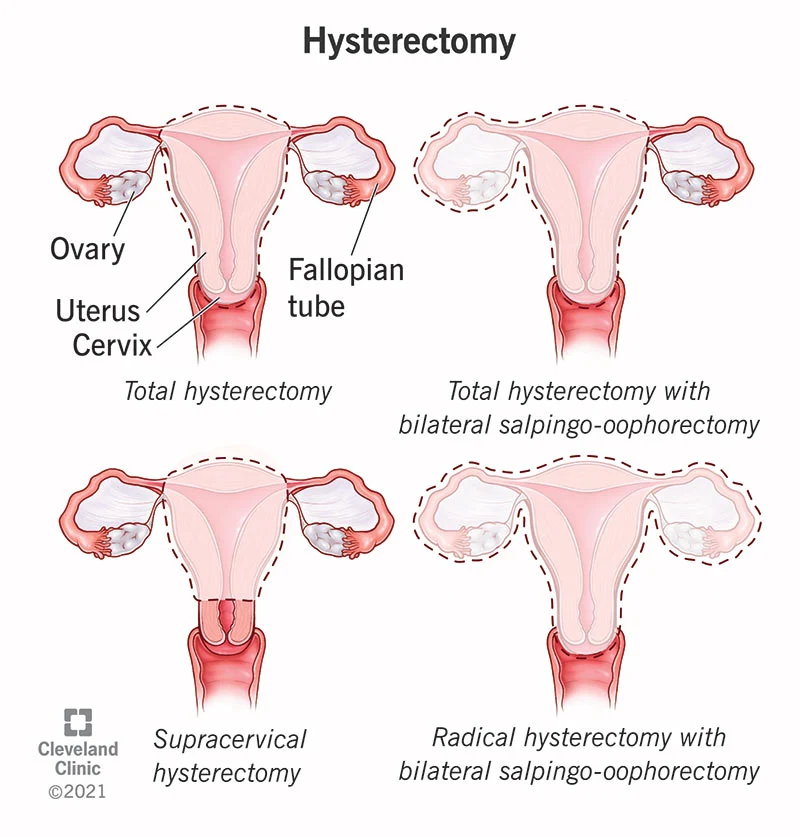
During this procedure, the surgeon removes the uterus (hysterectomy) along with the cervix, surrounding tissues, and sometimes the upper part of the vagina. Additionally, bilateral salpingo-oophorectomy involves the removal of both the fallopian tubes and the ovaries. This comprehensive surgical approach is typically recommended when there is a need to eliminate the primary source of estrogen production (the ovaries) and to ensure the removal of any potential cancerous or precancerous tissues, which might be present in the uterus or the surrounding structures.
It is a major surgery and can have significant implications for a person’s hormonal balance, reproductive capabilities, and overall health.
Common Reason for Radical Hysterectomy with Bilateral Salpingo-Oophorectomy
What are the effects after Radical Hysterectomy with Bilateral Salpingo-Oophorectomy?
How Long Does a Radical Hysterectomy with Bilateral Salpingo-Oophorectomy Take?
Laparoscopy in Radical Hysterectomy with Bilateral Salpingo-Oophorectomy: A Minimally Invasive Surgical Approach
New York Gynecology Surgery & Endometriosis (NYGSE) Approach
Why would my surgeon remove my ovaries with a hysterectomy?
Removing ovaries can prevent cancer spread and eliminate hormone-driven risk; the choice depends on cancer type, stage, age and genetic risk.
How long does full recovery take?
Most patients take 6–12 weeks for full recovery; light activity resumes earlier per surgeon instructions.
Will I go into menopause after this surgery?
Yes, removing both ovaries causes immediate surgical menopause with possible hot flashes, vaginal dryness and longer‑term bone/heart considerations.
Can I use hormone replacement therapy (HRT) after surgery?
Many patients can use HRT to treat menopausal symptoms, but safety depends on cancer type and medical history — discuss before surgery.
Will this surgery affect my ability to have children?
Yes, natural pregnancy is no longer possible; fertility preservation (egg/embryo freezing) or fertility‑sparing procedures may be options before treatment.
Do you remove lymph nodes during this procedure?
Often lymph node assessment or removal is performed when indicated by tumor type and staging; the extent is decided by your surgeon.
What are the main risks and complications?
Risks include bleeding, infection, urinary or bowel injury, blood clots and menopausal effects; serious complications are uncommon but discussed preoperatively.
Are minimally invasive approaches available (robotic or laparoscopic)?
Yes, when clinically appropriate we offer laparoscopic/robotic approaches that may reduce blood loss and speed recovery.
When should I call the clinic after surgery?
Call for fever >101°F, heavy bleeding, persistent or worsening pain, shortness of breath, or any sudden concerning symptoms at the incision or systemically.
What should I expect in the first 6–12 weeks after surgery?
Early weeks: hospital stay 1–3 days, walk soon after surgery, pain controlled with meds; weeks 2–6: energy returns, avoid heavy lifting; weeks 6–12: gradual return to full activity and follow‑up care.

Total Hysterectomy with Bilateral Salpingo-Oophorectomy
What is a Total Hysterectomy With Bilateral Salpingo-Oophorectomy?
A total hysterectomy with bilateral salpingo-oophorectomy is a comprehensive surgical procedure performed on individuals, primarily women, to remove the uterus, cervix, fallopian tubes, and both ovaries. This surgery is often recommended to treat various gynecological conditions such as uterine fibroids, endometriosis, gynecological cancers, and severe pelvic inflammatory disease.
The removal of these reproductive organs results in permanent infertility and typically induces menopause if the ovaries are removed, as they are responsible for hormone production. While this procedure can alleviate symptoms and effectively treat underlying conditions, it also has profound implications for a person’s reproductive and hormonal health.
What are the most common reasons for a total hysterectomy with bilateral salpingo-oophorectomy?
What are the effects after Total Hysterectomy with Bilateral Salpingo-Oophorectomy?
How Long Does a Total Hysterectomy with Bilateral Salpingo-Oophorectomy Take?
The duration of a total hysterectomy with bilateral salpingo-oophorectomy varies depending on factors such as the surgical approach and complexity of the case, but on average, it typically takes about 1 to 3 hours to complete.
Minimally invasive techniques, like laparoscopic or robotic-assisted procedures, tend to have shorter operating times than traditional open surgeries.
The surgeon’s experience and the patient’s overall health also play a role in determining the length of the surgery.
Dr. Pankaj Singhal is widely regarded and respected as a Master Surgeon in Robotic Surgeries, having performed over 10,000 robotic gynecologic, endometriosis, and cancer procedures, further emphasizing his expertise and proficiency in this field.
Laparoscopy in Total Hysterectomy with Bilateral Salpingo-Oophorectomy: A Minimally Invasive Surgical Approach
Laparoscopy, a minimally invasive surgical technique, has become a valuable approach in performing total hysterectomy with bilateral salpingo-oophorectomy. During this procedure, the surgeon makes small incisions in the abdominal wall through which specialized instruments and a laparoscope are inserted. The laparoscope is equipped with a camera that provides a magnified view of the pelvic and abdominal organs on a monitor, allowing for precise and controlled surgical maneuvers.
One of the primary benefits of laparoscopy in this context is its ability to minimize the invasiveness of the surgery. Compared to traditional open surgery, laparoscopy typically results in smaller incisions, reduced blood loss, and a lower risk of infection. Patients who undergo laparoscopic total hysterectomy with bilateral salpingo-oophorectomy often experience shorter hospital stays, faster recovery times, and less postoperative pain.
New York Gynecology Surgery & Endometriosis (NYGSE) Approach
Facing a Total Hysterectomy with Bilateral Salpingo-Oophorectomy can be a challenging and emotionally charged experience. At NYGSE, our commitment is to deliver personalized care that caters to your specific needs. Our team comprises experienced gynecologists and healthcare professionals who will stand by you throughout this journey, offering unwavering support, addressing your questions, and ensuring your comfort at every stage.
Your well-being remains our utmost priority, and we are dedicated to surpassing your expectations by providing top-quality care and individualized attention. If you or someone you care about is contemplating or has a scheduled Total Hysterectomy with Bilateral Salpingo-Oophorectomy or has any concerns related to this procedure, please do not hesitate to contact us.
We are here to offer guidance and assistance as you navigate this crucial decision-making process and embark on your treatment path.
NYGSE offers total hysterectomy with bilateral salpingo-oophorectomy for patients throughout Babylon and Bay Shore, NY, providing experienced surgical care in a setting focused on comfort, safety, and long-term health.
How is a total hysterectomy with bilateral salpingo-oophorectomy different from a standard hysterectomy?
A “standard” hysterectomy typically means removing the uterus (often including the cervix) while leaving the fallopian tubes and ovaries in place. A total hysterectomy with bilateral salpingo‑oophorectomy removes the uterus, both fallopian tubes and both ovaries. The key consequences are hormonal and reproductive: removing the ovaries causes immediate surgical menopause in premenopausal people, with symptoms (hot flashes, vaginal dryness, mood changes) and longer‑term effects on bone and heart health—so hormone therapy and other preventive measures may be discussed. Fertility is eliminated in either case, but only the oophorectomy produces the abrupt loss of ovarian hormones. Surgery and recovery are broadly similar, though adding removal of tubes and ovaries can modestly increase operative time and influence long‑term health decisions; the choice is guided by cancer risk, symptoms, age, and patient preference.
Why would the ovaries and fallopian tubes be removed during a total hysterectomy?
A total hysterectomy removes the uterus and cervix. When bilateral salpingo-oophorectomy is added, both fallopian tubes and both ovaries are also removed. This may be recommended for certain cancers, high inherited cancer risk, advanced endometriosis, ovarian disease, or other conditions where keeping the ovaries could leave future health risks. The decision depends on diagnosis, age, symptoms, cancer risk, and long-term hormonal health.
What is the difference between a hysterectomy, salpingectomy, oophorectomy, and bilateral salpingo-oophorectomy?
A hysterectomy removes the uterus, and a total hysterectomy also removes the cervix. A salpingectomy removes one or both fallopian tubes. An oophorectomy removes one or both ovaries. A bilateral salpingo-oophorectomy removes both fallopian tubes and both ovaries. When all of these are performed together, the procedure may be called a total hysterectomy with bilateral salpingo-oophorectomy.
Will I go into menopause after a total hysterectomy with bilateral salpingo-oophorectomy?
Yes, if both ovaries are removed before natural menopause, the patient enters surgical menopause because the ovaries are no longer producing the same levels of estrogen and other hormones. Symptoms may include hot flashes, night sweats, vaginal dryness, sleep changes, mood changes, and changes in sexual function. Cleveland Clinic also notes that removing the ovaries starts menopause immediately if menopause has not already occurred.
Is hormone therapy needed after a total hysterectomy with BSO?
Hormone therapy may be discussed after surgery, especially for patients who have both ovaries removed before natural menopause. Whether it is appropriate depends on the reason for surgery, cancer history or risk, age, symptoms, and overall health. This should be reviewed with the surgeon or treating physician before surgery so the patient understands both symptom management and long-term health considerations.
What are the long-term health considerations after ovary removal?
Removing both ovaries before natural menopause may affect bone health, heart health, sexual health, and menopausal symptoms. ACOG notes that bilateral salpingo-oophorectomy causing surgical menopause reduces ovarian cancer risk but may increase the risk of issues such as cardiovascular disease, osteoporosis, cognitive impairment, and all-cause mortality in some patients.
Can a total hysterectomy with bilateral salpingo-oophorectomy be done laparoscopically or robotically?
In many cases, yes. A laparoscopic or robotic-assisted approach may be possible depending on the patient’s condition, anatomy, prior surgeries, cancer concerns, endometriosis severity, and surgeon evaluation.
How long is recovery after a total hysterectomy with BSO?
Recovery depends on the surgical approach and the complexity of the case. Minimally invasive procedures often involve smaller incisions and a shorter recovery than open abdominal surgery, but patients still need time to heal internally.
Are there alternatives to total hysterectomy with bilateral salpingo-oophorectomy?
Sometimes. Alternatives depend on the diagnosis. For benign conditions, options may include medication, hormone therapy, endometriosis excision, myomectomy, ovarian cyst treatment, or hysterectomy without ovary removal. For cancer or high-risk genetic situations, surgery may be the safest recommendation.
Is total hysterectomy with BSO used for endometriosis?
It may be considered in select cases of severe or advanced endometriosis, especially when symptoms are debilitating or other treatments have not been successful. However, endometriosis care is highly individualized, and removing the uterus and ovaries is not automatically the right choice for every patient. This should be evaluated by a surgeon experienced in complex endometriosis and pelvic surgery.
What questions should I ask before having a total hysterectomy with bilateral salpingo-oophorectomy?
Patients may want to ask why each organ is being removed, whether the ovaries can be preserved, whether the surgery can be done laparoscopically or robotically, what recovery will involve, whether hormone therapy may be needed, how surgical menopause will be managed, and what long-term follow-up is recommended.
Laparoscopic Hysterectomy
What Is a Laparoscopic Hysterectomy?
What are the Advantages of Laparoscopic Hysterectomy?
How Long Does a Hysterectomy Take?
Laparoscopic Hysterectomy Using Robotic Surgery with the da Vinci Surgical System: A Minimally Invasive Surgical Approach
Laparoscopic hysterectomy using robotic surgery with the da Vinci Surgical System offers advanced and precise minimally invasive surgical options for patients. This innovative approach combines the benefits of traditional laparoscopic surgery with the enhanced capabilities of robotic technology. During the procedure, the surgeon operates from a console, controlling robotic arms that hold and manipulate surgical instruments with exceptional precision. The robotic system provides a 3D high-definition view of the surgical area, allowing for improved visualization and dexterity, making it an excellent choice for complex cases or when the utmost surgical precision is required.
One key advantage of the da Vinci system is the potential for shorter hospital stays and quicker recovery times compared to open surgery. The smaller incisions result in less post-operative pain, reduced scarring, and a faster return to daily activities for patients. Additionally, the robotic technology minimizes hand tremors, allowing for steady and meticulous movements during the procedure. While da Vinci-assisted laparoscopic hysterectomy can be more costly than traditional approaches, many patients and surgeons find that the potential benefits in terms of reduced pain and a faster return to normal life make it a valuable option for certain cases.

New York Gynecology Surgery & Endometriosis (NYGSE) Approach
Who is a candidate for minimally invasive hysterectomy?
A minimally invasive hysterectomy (laparoscopic, robotic-assisted, or vaginal) can be an excellent option for many people who need definitive surgical treatment of uterine or gynecologic conditions. Ideal candidates typically include those who:
Have benign gynecologic conditions such as:
- Symptomatic uterine fibroids (especially when symptoms - bleeding, pain, bulk - are not controlled by medical therapy)
- Abnormal uterine bleeding unresponsive to medical management
- Adenomyosis causing pain or heavy bleeding
- Chronic pelvic pain attributable to the uterus
- Recurrent or severe endometrial hyperplasia (without invasive cancer)
- Uterine prolapse (vaginal hysterectomy often favored)
- Severe pelvic inflammatory disease sequelae when conservative measures fail
- Need removal of the uterus for early-stage, well-selected gynecologic cancers (e.g., some cases of early endometrial cancer) when oncologic criteria allow minimally invasive approaches.
- Want the benefits of minimally invasive surgery: smaller incisions, less blood loss, shorter hospital stay, faster recovery, and less postoperative pain—provided their anatomy and medical condition are suitable.
Patient- and procedure-specific factors that support candidacy
- Uterine size and shape: Many surgeons can perform minimally invasive hysterectomy for moderately enlarged uteri (e.g., fibroid uteri), though very large uteri or extreme distortion may favor an open approach.
- Body habitus: Obesity is not an absolute contraindication; many obese patients successfully undergo laparoscopic or robotic hysterectomy, though surgeon experience and equipment matter.
- Prior abdominal or pelvic surgeries: Previous surgeries can cause adhesions that make minimally invasive approaches more challenging but not automatically impossible.
- Overall health: Patients should be medically optimized for anesthesia and surgery (e.g., controlled cardiac, pulmonary conditions); some serious comorbidities may increase operative risk and influence the approach.
- Desire for minimization of recovery time and wound complications.
Relative and absolute contraindications
- Absolute contraindications: Suspicion or confirmed advanced gynecologic malignancy requiring extensive open staging, uncontrolled bleeding or sepsis where emergent open surgery is safer.
- Relative contraindications: Extensive intra-abdominal adhesions, very large uterine size beyond surgeon capability, certain complex pelvic anatomy, severe cardiopulmonary disease that limits tolerance of pneumoperitoneum or Trendelenburg positioning. These are assessed individually.
Evaluation before deciding
- Thorough history and pelvic exam
- Pelvic ultrasound or other imaging (MRI/CT) to assess uterine size, fibroid burden, adnexal pathology
- Endometrial sampling if abnormal bleeding
- Medical optimization (e.g., anemia correction, management of comorbidities)
- Discussion of fertility wishes (hysterectomy is definitive - fertility ends)
- Counseling on risks, benefits, and alternative treatments (medical therapy, uterine-sparing procedures)
Shared decision-making
The best approach depends on diagnosis, uterine size and shape, prior surgeries, patient preferences, and surgeon experience. Minimally invasive hysterectomy is appropriate for many patients and often preferred when safe and feasible. Discuss personalized risks, expected recovery, and alternatives with your gynecologic surgeon.
How is robotic hysterectomy different from traditional laparoscopic hysterectomy?
Overview
Both are minimally invasive approaches to remove the uterus. They share the same goals (smaller incisions, less blood loss, faster recovery than open surgery) but differ in the technology and surgeon interface.
Key technical differences
Surgeon interface:
- Robotic: Surgeon sits at a console and controls robotic arms; instruments have wristed, multi‑degree articulation that mimic hand movements.
- Laparoscopic: Surgeon stands at the bedside and manipulates long, rigid instruments directly.
- Visualization:
- Robotic: High‑definition, stable 3D magnified view of the pelvis.
- Laparoscopic: High‑definition 2D or 3D laparoscopes; traditionally 2D is common.
- Instrument movement and precision:
- Robotic: Tremor filtration, scaled motions, and wristed instruments allow finer movements in tight spaces.
- Laparoscopic: Instruments are less flexible (straight), requiring advanced manual dexterity and different hand–eye coordination.
Ergonomics and fatigue:
- Robotic: Improved ergonomics for the surgeon (seated console) and potentially less physical fatigue.
- Laparoscopic: More physically demanding for the surgeon (standing, awkward postures).
Setup and workflow:
- Robotic: Requires docking the robot and instrument exchanges through the system; longer setup time can occur.
- Laparoscopic: Faster setup in many hands; instrument exchanges at the bedside.
Clinical and outcome differences
- Operative time: Robotic cases may have longer total operating-room time (docking + console time), especially during the surgeon’s learning curve; some experienced teams achieve similar times.
- Blood loss, pain, hospital stay, recovery: Most studies show comparable patient outcomes between robotic and traditional laparoscopy for benign hysterectomy (similar blood loss, complication rates, length of stay, and return to activity).
- Conversion to open surgery: Some data suggest lower conversion rates with robotic surgery in complex cases (large uteri, adhesions), but results vary and depend on surgeon skill and case selection.
- Cost: Robotic hysterectomy is generally more expensive due to capital costs, maintenance, and disposable instruments.
- Learning curve: Robotic systems can shorten the learning curve for complex maneuvers compared with conventional laparoscopy for some surgeons, but competency still requires training and volume.
Indications
- Indications overlap completely; choice often depends on surgeon experience, case complexity (e.g., very large fibroid uterus, extensive adhesions), and institutional resources. Robotic systems may be favored for technically challenging anatomy where wristed instruments and 3D vision help.
Choosing between them
- Important factors: surgeon skill and experience with each approach, patient anatomy and comorbidities, complexity of disease, operating-room availability, and cost considerations.
- Outcomes are most influenced by appropriate case selection and surgeon proficiency rather than the platform alone.
Can laparoscopic hysterectomy be used for complex conditions like endometriosis or fibroids?
Yes–laparoscopic hysterectomy is commonly used to treat complex benign gynecologicconditions such as advanced endometriosis and symptomatic fibroid uteri, but appropriateness depends on disease extent, anatomy, and surgeon experience.
When it’s suitable
- Endometriosis: Laparoscopic hysterectomy (often combined with excision of endometriotic implants and adhesiolysis) is an effective option for severe, symptomatic disease when conservative management and fertility-sparing treatments have failed or are not desired. Laparoscopy allows direct visualization and targeted removal of implants in the pelvis.
- Fibroids: Many patients with fibroid-heavy or moderately enlarged uteri can undergo laparoscopic hysterectomy. Laparoscopy is feasible for multiple or intramural/subserosal fibroids; very large uteri or extreme distortion may favor alternative approaches (vaginal or open) or use of morcellation/dissection techniques as appropriate and safe.
Factors that influence choice
- Uterine size and shape: Very large uteri (extensive fibroid burden) increase technical difficulty and may require conversion to open or use of robotic assistance.
- Adhesions and distortion: Dense adhesions from prior surgery or severe endometriosis can lengthen surgery and increase conversion risk, but experienced laparoscopic surgeons often manage these laparoscopically.
- Involvement of other organs: Bowel, bladder, or ureteral involvement from deep infiltrating endometriosis may require multidisciplinary planning and possible open approach in complex cases.
- Surgeon skill and resources: Outcomes correlate strongly with surgeon experience and available equipment (advanced energy devices, robotics if needed).
- Patient comorbidities and preferences: Medical fitness for pneumoperitoneum/positioning and discussion about recovery, scarring, and fertility loss.
Benefits and risks
- Benefits: Minimally invasive approach usually yields less blood loss, smaller incisions, shorter hospital stay, faster recovery, and quicker return to activities compared with open hysterectomy.
- Risks: Longer operative time in complex cases, potential need for conversion to open surgery, and specific risks if adjacent organs are involved. For fibroids, morcellation has specific safety considerations if malignancy is a concern–preoperative evaluation is essential.
Preoperative evaluation and planning
- Imaging (ultrasound, MRI) to define fibroid size/location and endometriosis extent.
- Bowel/bladder evaluation and consultation with colorectal/urologic surgeons if organ involvement suspected.
- Medical optimization (anemia correction, comorbidity management).
- Clear counseling about alternatives (myomectomy, uterine-sparing therapies, medical/endometriosis-specific treatments) and about fertility implications (hysterectomy is definitive).
Bottom line
Laparoscopic hysterectomy is a valid and often preferred approach for many patients with complex fibroids or endometriosis when performed by experienced surgeons with appropriate preoperative planning; selected very large, extensively infiltrative, or multi‑organ cases may require robotic assistance or open surgery.
Supracervical Hysterectomy
Why Would a Doctor Recommend a Supracervical Hysterectomy?
What are the Most Common Reasons for Supracervical Hysterectomy?
What are the effects of removing the uterus in a Supracervical Hysterectomy?
How Long Does a Supracervical Hysterectomy Take?
Laparoscopy in Supracervical Hysterectomy: A Minimally Invasive Surgical Approach
New York Gynecology Surgery & Endometriosis (NYGSE) Approach
How is a supracervical hysterectomy different from a total hysterectomy?
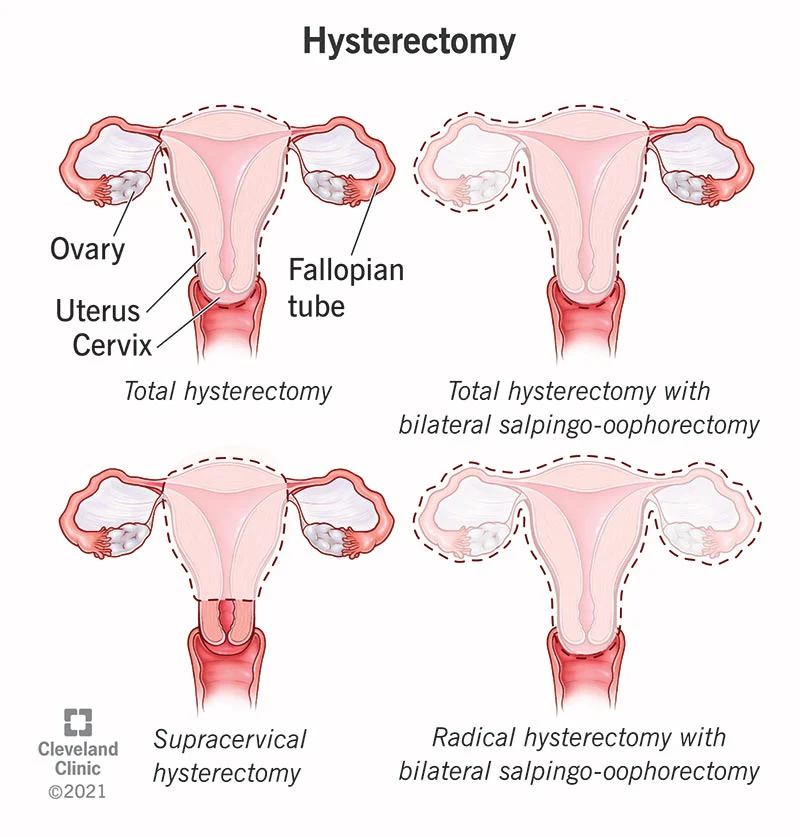
A supracervical (also called subtotal) hysterectomy and a total hysterectomy both remove the uterus, but the main difference is whether the cervix is taken out. In a supracervical procedure the uterine body is removed while the cervix is left in place; in a total hysterectomy the surgeon removes the entire uterus including the cervix.
That distinction has a few practical implications. With a supracervical hysterectomy there’s a small chance of ongoing bleeding or cyclic spotting if some endocervical tissue remains, and you will still need routine cervical screening (Pap/HPV) after surgery. A total hysterectomy eliminates the possibility of uterine-source bleeding and, if the cervix was normal and removed, usually means you no longer need cervical cancer screening.
From a recovery and complication standpoint, the two operations are broadly similar. Some studies suggest supracervical procedures can be slightly quicker with marginally less blood loss, but differences are generally small and depend on the surgeon and approach (vaginal, laparoscopic, or abdominal). Neither procedure reliably changes long-term sexual function or pelvic support in a consistent way.
Which is best comes down to the reason for surgery and patient preference. If there’s cervical dysplasia, cancer risk, or uncertainty about the cervix, a total hysterectomy is usually recommended. If the cervix is healthy and a patient prefers to keep it—and accepts the need for future screening and a small risk of bleeding—then a supracervical hysterectomy can be a reasonable option. In either case, decisions about removing ovaries or fallopian tubes are separate and affect hormone outcomes independently.
Hysterectomy
Why would a doctor recommend a hysterectomy?
A hysterectomy, which involves the surgical removal of the uterus, ranks as the second most frequent surgical procedure for females, following closely behind cesarean section (C-section).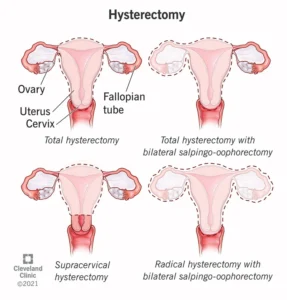
Data from the Centers for Disease Control and Prevention (CDC) reveals that the United States boasts the highest rate of hysterectomy surgeries globally, with an annual count exceeding 600,000. Further statistics indicate that approximately 20 million American women have undergone a hysterectomy, and it is estimated that about one in every three women will experience this procedure by the time they reach the age of 60.
There are several medical reasons why a hysterectomy may be recommended by a healthcare provider. Some of the common indications for a hysterectomy include:
- Uterine Fibroids: These are benign growths in the uterus that can lead to heavy menstrual bleeding, pelvic discomfort, and pressure on nearby organs. When fibroids reach a significant size or cause substantial symptoms, a hysterectomy may be considered as a treatment option.
- Endometriosis: This condition involves tissue similar to the uterine lining growing outside the uterus. Severe cases of endometriosis that do not respond to alternative treatments may necessitate a hysterectomy.
- Uterine Prolapse: This occurs when the uterus descends into the vaginal canal, causing discomfort, pelvic pressure, and urinary incontinence. In certain instances, a hysterectomy may be required to correct this condition.
- Chronic Pelvic Pain: When persistent pelvic pain believed to be linked to the uterus does not respond to other therapies, a hysterectomy may be suggested as a final recourse.
- Adenomyosis: This condition involves the endometrial tissue growing into the muscular wall of the uterus, leading to heavy bleeding and pain. In severe cases, a hysterectomy may be an option.
- Uterine Cancer: If cancer is detected within the uterus, a hysterectomy may be performed as part of the treatment, often in conjunction with other treatments like radiation or chemotherapy.
- Abnormal Uterine Bleeding: Excessive or irregular menstrual bleeding that remains unresponsive to other treatments may result in a hysterectomy to alleviate symptoms and address underlying concerns.
- Pelvic Inflammatory Disease (PID): In cases of severe PID that do not improve with antibiotics and other therapies, a hysterectomy may be recommended to prevent the spread of infection and safeguard overall health.
- Preventive Measures: In some cases, a hysterectomy may be considered as a preventive measure for women with a strong family history of uterine or ovarian cancer, or if they have a genetic predisposition to these conditions.
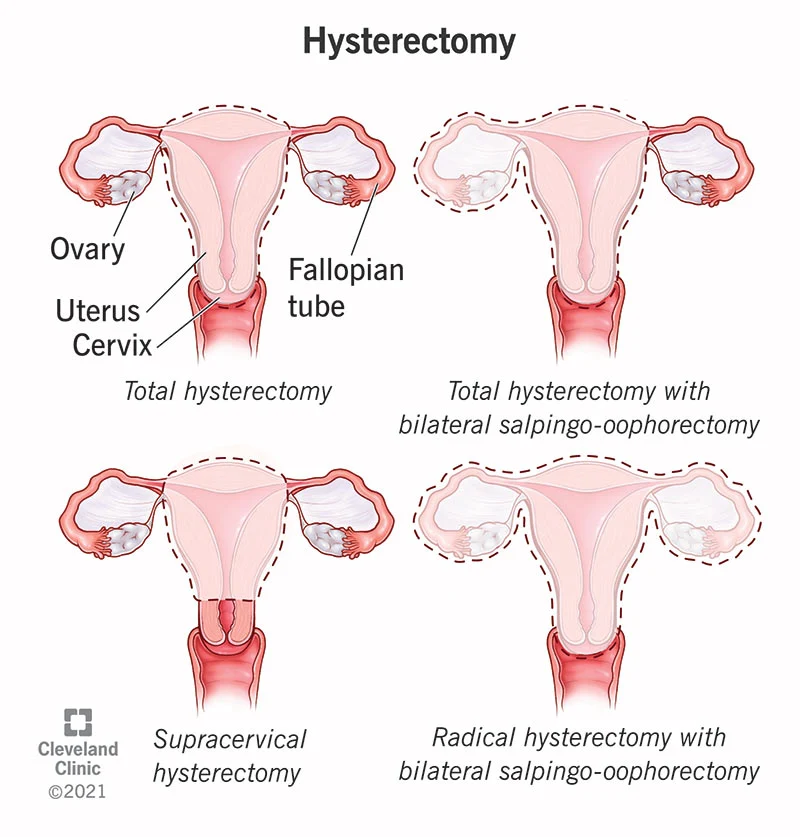
What are the different types of hysterectomy?
How Long Does a Hysterectomy Take?
What is laparoscopic hysterectomy and how does it work?
New York Gynecology Surgery & Endometriosis (NYGSE) Approach
What is the difference between a hysterectomy and a laparoscopic hysterectomy?
A hysterectomy is the surgical procedure itself (removal of the uterus), while laparoscopic hysterectomy refers to the specific technique used to perform the surgery.
Key Differences:
Hysterectomy Types by Approach:
- Open hysterectomy: Large abdominal incision (5-7 inches)
- Laparoscopic hysterectomy: 3-4 small incisions (0.5-1 inch each) using a camera and specialized instruments
- Vaginal hysterectomy: Removal through the vagina with no external incisions
- Robotic-assisted laparoscopic hysterectomy: Enhanced precision using robotic technology
Laparoscopic Hysterectomy Benefits:
- Smaller incisions and minimal scarring
- Faster recovery time (2-4 weeks vs. 6-8 weeks)
- Less post-operative pain
- Reduced risk of infection
- Shorter hospital stay (often same-day or overnight)
- Quicker return to normal activities
Recovery Comparison:
Open hysterectomy: 6-8 weeks full recovery
Laparoscopic hysterectomy: 2-4 weeks full recovery
Candidacy:
Not all patients are candidates for laparoscopic approach. Factors include uterine size, previous surgeries, and specific medical conditions.
Bottom line: Laparoscopic hysterectomy is a minimally invasive technique for performing a hysterectomy, offering significant advantages in recovery time and patient comfort compared to traditional open surgery.
Who is a candidate for minimally invasive hysterectomy?
Most women requiring hysterectomy are candidates for minimally invasive approaches (laparoscopic or robotic-assisted), but eligibility depends on specific medical factors and uterine characteristics.
Ideal Candidates Include Women With:
Medical Conditions:
- Uterine fibroids (small to moderate size)
- Endometriosis
- Abnormal uterine bleeding
- Uterine prolapse (mild to moderate)
- Chronic pelvic pain
- Precancerous cervical conditions
- Early-stage gynecologic cancers
Physical Characteristics:
- Uterine size less than 12-16 weeks gestational size
- Normal uterine mobility
- Adequate vaginal access
- No extensive pelvic adhesions
Factors That May Require Open Surgery:
Contraindications:
- Very large uterus (>16-20 weeks size)
- Extensive endometriosis with severe adhesions
- History of multiple abdominal surgeries
- Suspected advanced cancer requiring extensive staging
- Certain heart or lung conditions
- Inability to tolerate general anesthesia positioning
Relative Contraindications:
- Obesity (BMI >40) - case-by-case evaluation
- Previous cesarean sections (may increase complexity)
- Large ovarian masses
Success Rates:
- 85-90% of hysterectomies can be performed minimally invasively
- Success depends on surgeon experience and patient factors
Evaluation Process:
Your gynecologic surgeon will assess your specific case through physical examination, imaging studies, and medical history to determine the best surgical approach.
Bottom line: Most women are candidates for minimally invasive hysterectomy, with patient selection based on uterine size, medical conditions, and individual anatomy.
When should you see a gynecologic surgeon for hysterectomy on Long Island?
You should consult a gynecologic surgeon when conservative treatments have failed to address severe gynecologic conditions that significantly impact your quality of life, or when immediate surgical intervention is medically necessary.
Immediate Consultation Required:
Urgent Conditions:
- Heavy bleeding causing anemia or requiring blood transfusion
- Suspected gynecologic cancer
- Large fibroids causing severe symptoms
- Uterine prolapse interfering with daily activities
- Severe endometriosis unresponsive to medical management
Emergency Situations:
- Uncontrolled uterine bleeding
- Severe pelvic pain with suspected complications
- Signs of infection or sepsis
Consider Surgical Consultation When:
Failed Conservative Treatment:
- Hormonal therapies ineffective after 3-6 months
- Multiple medication trials unsuccessful
- Minimally invasive procedures (ablation, embolization) have failed
- Symptoms worsening despite treatment
Quality of Life Impact:
- Missing work/activities due to heavy periods
- Chronic pelvic pain affecting daily function
- Bladder/bowel problems from uterine prolapse
- Sexual dysfunction from gynecologic conditions
Specific Symptoms Warranting Evaluation:
Bleeding Issues:
- Periods lasting longer than 7 days
- Bleeding between periods
- Post-menopausal bleeding
- Soaking through protection hourly
Pain and Pressure:
- Severe menstrual cramps unrelieved by medication
- Chronic pelvic pressure or fullness
- Pain during intercourse
- Lower back pain from enlarged uterus
Long Island Considerations:
Access to Specialists:
- Board-certified gynecologic surgeons available
- Advanced minimally invasive techniques offered
- Multidisciplinary care teams
- Same-day consultation options available
Bottom line: See a gynecologic surgeon when symptoms significantly impact your life, conservative treatments have failed, or you have concerning symptoms requiring expert evaluation and potential surgical intervention.
