
November 19, 2025by admin
Stage 2 Endometriosis
Understanding the Stages 2 Endometriosis
Stage 2 endometriosis, also known as mild endometriosis, involves small but measurable implants of endometrial tissue on the pelvic lining and organs. Although the disease is still considered early-stage, the lesions are more numerous and slightly deeper than in Stage 1, and mild adhesions may be present. While symptoms can vary widely, many individuals with Stage 2 experience pelvic pain, menstrual discomfort, or early fertility challenges. The following sections explain the characteristics, symptoms, risks, and diagnostic criteria for Stage 2 endometriosis.
This chart shows how the rASRM scoring system defines Stage II endometriosis, considered mild disease.
Stage II reflects a greater number of implants than Stage I, with some being deeper, and mild adhesions may begin to appear. The system scores lesion size, depth, and the presence of early scar tissue to determine this classification.
Even though Stage II represents a mild level of spread, patient symptoms may be inconsistent and do not always match the staging severity.

COMMON QUESTIONS ABOUT Stage 2 Endometriosis
Stage 2 Endometriosis (Mild Endometriosis)
Stage 2 endometriosis is a classification within the four-stage system used to assess the severity of endometriosis, a chronic medical condition affecting individuals with female reproductive organs. In this stage, the condition is considered to be at a relatively moderate level of progression. It is characterized by the presence of minimal to mild implants of endometrial tissue outside the uterus and pelvic lining.
These implants, also known as lesions or growths, may be found on various pelvic organs and tissues, such as the ovaries, fallopian tubes, and the peritoneum (the lining of the abdominal cavity). Despite their presence outside the uterus, these endometrial tissue growths continue to respond to hormonal changes in the menstrual cycle, causing them to shed and bleed.
However, unlike more advanced stages of endometriosis, stage 2 is associated with fewer and smaller implants, and there may be less overall tissue involvement in the pelvic region. As with all stages of endometriosis, symptoms can vary widely, but they may include pelvic pain, painful menstrual periods, pain during intercourse, and infertility. Early diagnosis and appropriate management are crucial in order to alleviate symptoms and improve the quality of life for individuals with stage 2 endometriosis.
Symptoms of Stage 2 Endometriosis
Stage 2 endometriosis, characterized by minimal to mild implants of endometrial tissue outside the uterus and pelvic lining, can present with a range of symptoms that may vary from person to person. Common symptoms of stage 2 endometriosis may include:
- Pelvic Pain: Women with stage 2 endometriosis often experience pelvic discomfort or pain, which can be intermittent or chronic. The pain might be dull, sharp, or cramp-like and can worsen during menstruation, intercourse, or bowel movements.
- Painful Menstruation: Menstrual periods may be accompanied by more intense and prolonged cramps, often starting a few days before the period and lasting throughout its duration.
- Painful Intercourse: Pain or discomfort during sexual intercourse, known as dyspareunia, is a common symptom. It may be felt deep within the pelvis or lower abdomen.
- Gastrointestinal Symptoms: Some individuals might experience gastrointestinal issues such as bloating, constipation, diarrhea, or nausea, particularly around the time of their menstrual cycle.
- Fatigue: Chronic pain and other symptoms can contribute to feelings of fatigue and general tiredness.
- Infertility: Stage 2 endometriosis can affect fertility, as the abnormal tissue growths might interfere with the function of the ovaries, fallopian tubes, or uterus.
- Irregular Bleeding: Women with stage 2 endometriosis might experience irregular menstrual bleeding, spotting between periods, or heavy bleeding.
It’s worth highlighting that the intensity of symptoms is not always directly linked to the stage of endometriosis; individuals with stage 2 endometriosis can encounter varying degrees of symptom severity, ranging from significant discomfort to minimal effects.
If you suspect you may have endometriosis or are experiencing any symptoms of concern, it’s essential to request an appointment with New York Gynecology Surgery & Endometriosis (NYGSE) to seek medical advice and evaluation.
Life-threatening Complications in Stage 2 Endometriosis
While stage 2 endometriosis is generally considered to have a lower risk of life-threatening complications compared to more advanced stages, there are still potential concerns that individuals should be aware of. One notable risk is the potential impact on fertility. Even at this stage, endometriosis can lead to scarring and adhesions that may affect the reproductive organs, potentially leading to difficulties in conceiving and carrying a pregnancy to term.
Another concern is the possibility of severe and chronic pelvic pain. While not life-threatening in itself, this pain can significantly diminish an individual’s quality of life, potentially leading to mental health challenges and a decreased ability to engage in daily activities. Additionally, there is a small chance that endometrial tissue could attach to vital structures such as the intestines or bladder, potentially causing complications such as bowel obstruction or urinary issues. While these risks are relatively uncommon at stage 2, it’s important for individuals with endometriosis to stay informed, seek medical guidance, and explore appropriate treatment options to manage their condition and minimize potential complications.
Diagnosis of Stage 2 Endometriosis
Diagnosing stage 2 endometriosis involves:
- Clinical Assessment: Your healthcare provider will gather your medical history and discuss your symptoms, focusing on menstrual patterns, pelvic pain, and other relevant information.
- Physical Examination: A pelvic exam may be conducted to check for tender areas, masses, or other signs of endometriosis.
- Imaging: Ultrasound or MRI scans may be used to visualize pelvic structures, helping identify possible endometriosis-related abnormalities.
- Laparoscopy: Considered the definitive diagnostic method, a minimally invasive surgical procedure (laparoscopy) allows direct visualization of pelvic organs, enabling the doctor to identify and evaluate endometriosis lesions. Biopsies can be taken for confirmation.
Early diagnosis and intervention can lead to more effective management and improved quality of life for individuals with endometriosis.
Service Areas
Women in Babylon and Bay Shore, NY diagnosed with Stage 2 endometriosis turn to NYGSE for thoughtful evaluation and targeted treatment, with care plans designed to manage symptoms and slow progression close to home.
Surgical Treatment for Stage 2 Endometriosis
A common surgical treatment for stage 2 endometriosis is laparoscopic excision or removal of endometrial tissue growths. This minimally invasive procedure aims to alleviate symptoms, improve quality of life, and potentially enhance fertility.
Here’s how surgical treatment for Stage 2 endometriosis is usually conducted:
Laparoscopy
Laparoscopy is a widely employed treatment for stage 2 endometriosis, a condition characterized by minimal to mild implants of endometrial tissue outside the uterus and pelvic lining. This minimally invasive surgical procedure serves a dual purpose of diagnosis and intervention.
During laparoscopy, a small incision is made near the navel, through which a thin tube with a camera (laparoscope) is inserted. The surgeon utilizes real-time visual guidance to examine the pelvic region, confirming the presence and extent of endometrial tissue growths. Upon identification, the surgeon can delicately excise or ablate these growths, removing abnormal tissue, adhesions, and cysts as needed. By addressing these tissue implants, laparoscopy aims to alleviate symptoms such as pelvic pain, painful menstruation, and discomfort during intercourse that often accompany stage 2 endometriosis. Its minimally invasive nature generally leads to quicker recovery times, reduced postoperative pain, and decreased scarring compared to traditional open surgery.
Following laparoscopy, a tailored treatment plan, potentially including pain management and hormonal therapies, may be recommended to manage symptoms and prevent recurrence, ensuring improved quality of life for individuals with stage 2 endometriosis.
According to Healthcare Bluebook, the cost of laparoscopic excision of endometriosis can vary depending on the location, healthcare provider, and type of insurance. On average, the cost of the procedure can range from $4,000 to $15,000. It’s important to note that these are estimated costs and may not reflect the actual cost you may incur.
To obtain an accurate cost estimate, it is advisable to request an appointment with NYGSE.
Excision or Ablation
When addressing stage 2 endometriosis, two primary surgical options are excision and ablation, both aimed at removing or destroying endometrial tissue growths outside the uterus. Excision involves the meticulous removal of these growths, along with any associated scar tissue or adhesions. This method aims to fully eliminate the abnormal tissue, potentially providing more comprehensive relief from symptoms like pelvic pain, while also reducing the risk of recurrence. Excision is often preferred when the goal is to achieve long-term symptom management and enhance fertility, as it addresses the underlying tissue involvement.
In contrast, ablation employs techniques like heat or laser to destroy the endometrial tissue growths. While less invasive than excision, ablation may not completely eliminate all abnormal tissue, potentially leaving behind microscopic implants.
Robotic Surgery
Robotic surgery is emerging as an advanced and minimally invasive option for treating stage 2 endometriosis, characterized by minimal to mild endometrial tissue growths outside the uterus and pelvic lining. This technique involves the use of robotic-assisted surgical systems, where a surgeon controls robotic arms equipped with surgical instruments to perform precise and intricate procedures. Robotic surgery offers enhanced dexterity, visualization, and maneuverability, making it well-suited for addressing endometriosis lesions with precision.
During robotic surgery for stage 2 endometriosis, small incisions are made to insert robotic arms and a high-definition camera into the abdomen. The surgeon controls the robotic arms from a console, guiding them to remove endometrial tissue growths and address any adhesions or scar tissue. This minimally invasive approach often leads to reduced postoperative pain, shorter hospital stays, and quicker recovery compared to traditional open surgery. Robotic surgery’s increased precision can aid in sparing healthy tissue and minimizing potential damage to surrounding structures, which is particularly advantageous when treating stage 2 endometriosis to alleviate symptoms like pelvic pain, painful periods, and fertility issues.

Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Expert treatment. Compassionate care. Real results.
November 18, 2025by admin
Stage 1 Endometriosis
Understanding the Stages 1 Endometriosis
Stage 1 endometriosis, also called minimal endometriosis, represents the earliest form of the disease. At this stage, tiny superficial implants are present on the pelvic lining or ovaries with little to no scar tissue. Although considered the least severe classification, Stage 1 can still cause symptoms, discomfort, or fertility challenges in some individuals. The following overview explains how Stage 1 endometriosis is identified, what symptoms may occur, and how it is typically diagnosed and managed.
This chart illustrates how the revised American Society for Reproductive Medicine (rASRM) scoring system classifies Stage I endometriosis, also known as minimal disease.
Stage I includes a few small, superficial implants with little to no scar tissue. The scoring reflects the limited size and depth of lesions and the absence of significant adhesions or endometriomas.
While this stage indicates the least extensive disease, symptoms can still vary widely — some patients experience pain, while others have no symptoms at all.
COMMON QUESTIONS ABOUT Stage 1 Endometriosis
Stage 1 Endometriosis (Minimal Endometriosis)
Stage 1 endometriosis, also known as minimal endometriosis, is the earliest and least severe form of the condition. In this stage, small patches or isolated implants of endometrial tissue are found outside the uterus, typically on the pelvic lining or ovaries. These implants are small and superficial, measuring only a few millimeters in size. At this stage, there is minimal scarring or adhesion formation.
Despite being classified as the least severe, stage 1 endometriosis can still cause symptoms and discomfort for some individuals. Common symptoms include mild pelvic pain, particularly during menstruation, and possibly pain during intercourse. However, some women with stage 1 endometriosis may have no noticeable symptoms at all.
Diagnosing stage 1 endometriosis typically involves a laparoscopy, a minimally invasive surgical procedure, during which a thin tube with a camera is inserted into the abdomen to visualize and assess the pelvic structures. If stage 1 endometriosis is detected, appropriate management options may include pain medication, hormonal therapy, or lifestyle changes. It’s crucial for individuals experiencing symptoms or fertility concerns to consult with a healthcare professional for a comprehensive evaluation and personalized treatment plan. Early detection and management can help minimize the impact of the condition on a person’s overall health and quality of life.
Symptoms of Stage 1 Endometriosis
Stage 1 endometriosis is the mildest form of the condition, and noticeable symptoms may not always be present. However, some individuals with stage 1 endometriosis may experience the following symptoms:
- Mild Pelvic Pain: Women may experience mild, intermittent pelvic pain or discomfort, especially during menstruation (dysmenorrhea). The pain can vary from person to person and may be felt in the lower abdomen or back.
- Pain During Intercourse: Some women with stage 1 endometriosis may have pain or discomfort during or after sexual intercourse (dyspareunia).
- Mild Menstrual Irregularities: Menstrual cycles may be slightly irregular, with variations in flow or length.
- Fatigue: Fatigue or tiredness may occur during menstruation due to hormonal changes and pain.
Importantly, some individuals with stage 1 endometriosis may have no noticeable symptoms and may only discover the condition incidentally during medical evaluations for other concerns, such as infertility investigations.
It’s crucial to understand that the severity and presentation of symptoms can differ significantly among individuals.
Additionally, some women may have stage 1 endometriosis and experience severe pain, while others with more advanced stages may have milder symptoms.
If you suspect you may have endometriosis or are experiencing any symptoms of concern, it’s essential to request an appointment with New York Gynecology Endometriosis (NYGE) to seek medical advice and evaluation.
Life-threatening Complications in Stage 1 Endometriosis
In Stage 1 endometriosis, life-threatening complications are rare because the disease is in its early and least severe form. However, it’s important to note that endometriosis, regardless of its stage, can cause various health challenges and negatively impact a person’s quality of life. While life-threatening complications are not typically associated with Stage 1 endometriosis, the condition can progress over time and may lead to more severe symptoms or fertility issues if left untreated.
It’s crucial for individuals with endometriosis to seek medical attention, adhere to their healthcare provider’s recommendations, and actively manage the condition to prevent potential complications in the future. Regular follow-ups with a healthcare professional can help monitor the progression of the disease and address any emerging concerns.
Diagnosis of Stage 1 Endometriosis
The diagnosis of Stage 1 endometriosis typically involves a combination of the following steps:
- Medical History: Your healthcare provider will begin by taking a detailed medical history, including asking about your symptoms, menstrual cycle, and any previous medical conditions or surgeries.
- Physical Examination: A pelvic examination may be performed to check for any abnormalities or signs of endometriosis.
- Imaging Studies: While Stage 1 endometriosis may not always be visible on imaging, an ultrasound may be conducted to rule out other possible causes of pelvic pain and to assess the pelvic structures.
- Laparoscopy: The gold standard for diagnosing endometriosis is through a surgical procedure called laparoscopy. During laparoscopy, a thin, lighted instrument (laparoscope) is inserted through a small incision in the abdomen to visualize the pelvic organs and look for endometrial implants, lesions, or adhesions. Biopsies of suspicious areas may be taken for further confirmation.
- Histology: Biopsy samples obtained during laparoscopy are sent to a pathologist for examination under a microscope to confirm the presence of endometrial tissue outside the uterus.
Early diagnosis and intervention can lead to more effective management and improved quality of life for individuals with endometriosis.
Service Areas
NYGSE provides care for patients across Babylon and Bay Shore, NY experiencing Stage 1 endometriosis, focusing on early intervention, accurate diagnosis, and personalized treatment strategies that address symptoms before they become more advanced.
Surgical Treatment for Stage 1 Endometriosis
Surgical treatment for Stage 1 endometriosis typically involves a minimally invasive procedure called laparoscopy. The main goals of surgical treatment are to diagnose the condition definitively and to remove or ablate (destroy) any endometrial implants or lesions found during the procedure.
Here’s how surgical treatment for Stage 1 endometriosis is usually conducted:
Laparoscopy
Laparoscopic surgery is performed under general anesthesia. A small incision is made near the navel, and a thin, lighted instrument called a laparoscope is inserted to visualize the pelvic organs and identify endometrial implants.
According to Healthcare Bluebook, the cost of laparoscopic excision of endometriosis can vary depending on the location, healthcare provider, and type of insurance. On average, the cost of the procedure can range from $4,000 to $15,000. It’s important to note that these are estimated costs and may not reflect the actual cost you may incur.
To obtain an accurate cost estimate, it is advisable to request an appointment with New York Gynecology Surgery & Endometriosis (NYGSE).
Excision or Ablation
In Stage 1 endometriosis, both excision and ablation are possible surgical treatment options, depending on the specific characteristics of the endometrial lesions and the surgeon’s expertise. Here’s an explanation of each procedure:
- Excision: Excision involves surgically removing the endometrial lesions or implants. The surgeon carefully cuts away the affected tissue, ensuring that the entire lesion is removed, including any deep-seated parts. This method aims to completely eliminate the endometriotic tissue, reducing the likelihood of recurrence.
- Ablation: Ablation, also known as vaporization or coagulation, uses heat (laser or electrical energy) to destroy the endometrial lesions. The heat energy effectively destroys the tissue on the surface, but it may not penetrate deeply into the lesion. As a result, there is a higher chance of residual tissue remaining, which can potentially lead to a higher chance of recurrence compared to excision.
While both excision and ablation can be used for Stage 1 endometriosis, excision is generally considered more effective for completely removing the endometrial tissue and reducing the risk of recurrence. However, the choice of the surgical technique depends on various factors, including the size and location of the lesions, the surgeon’s expertise, and the individual patient’s preferences and needs.
Robotic Surgery
Robotic surgery is an advanced and minimally invasive approach for treating Stage 1 endometriosis. During the procedure, small incisions are made in the abdomen, and a robotic surgical system is used to control precise movements of surgical instruments. The surgeon can visualize the pelvic organs in high-definition 3D, identify and remove or ablate endometrial implants, and potentially address any adhesions. Robotic surgery offers advantages such as improved precision, reduced tissue trauma, shorter hospital stays, and potentially faster recovery compared to traditional open surgery.
However, the choice of surgical approach should be discussed with a qualified healthcare professional based on individual needs and circumstances.
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Have Questions About Your Surgery or Treatment?
Expert treatment. Compassionate care. Real results.
November 18, 2025by admin
Pelvic Adhesions
Understanding Pelvic and Abdominal Adhesions?
Pelvic and abdominal adhesions are bands of scar-like tissue that cause organs or tissues to stick together abnormally. While adhesions can form after infection or surgery, endometriosis is now recognized as the most common cause. Unlike post-surgical adhesions—which are typically made of fibrous scar tissue alone—endometriosis adhesions contain active glands, stroma, inflammation, and fibrosis, making them more complex, more painful, and more likely to distort pelvic anatomy. These adhesions can involve the ovaries, uterus, bowel, bladder, pelvic sidewalls, and more, often contributing to chronic pelvic pain, infertility, and organ dysfunction.
Laparoscopic image showing thin, transparent, fibrous bands of endometriosis-related adhesions connecting pelvic organs. The adhesions appear stretched and vascular, consistent with inflammatory endometriosis tissue rather than simple post-surgical scar tissue.
COMMON QUESTIONS ABOUT Pelvic and Abdominal Adhesions?
How do Adhesions Form?
Adhesions can form due to various causes such as inflammation, infection, trauma, surgery, or endometriosis, resulting in the abnormal formation of fibrous bands or scar tissue in the pelvic or abdominal cavity.
(a) Endometriosis Adhesions
Endometriosis is a condition in which the tissue that normally lines the inside of the uterus, called the endometrium, grows outside of the uterus, typically in the pelvic cavity. This can result in the formation of adhesions, which are fibrous bands or scar tissue that can occur as a secondary response to the inflammatory process associated with endometriosis.
When endometrial tissue implants on pelvic organs, such as the ovaries, fallopian tubes, bladder, or intestines, it can cause irritation, inflammation, and tissue damage. Over time, the body’s healing response may involve the formation of scar tissue or fibrous bands in an attempt to repair the damaged tissue. However, this scar tissue can also stick to nearby organs and tissues, leading to the formation of adhesions.
(b) Adhesions secondary to surgery
Adhesions that occur as a secondary result of surgery are fibrous bands or scar tissue that can form in the abdominal or pelvic cavity as a natural part of the body’s healing response to surgical intervention. Surgery, particularly abdominal or pelvic surgery, can result in tissue trauma, inflammation, and disruption of normal tissue planes, leading to the formation of adhesions during the healing process.
After surgery, the body undergoes a process of tissue repair, which involves the deposition of collagen, a fibrous protein, to help heal the surgical incision or injured tissues. However, in some cases, this healing process can result in the formation of excessive scar tissue or adhesions. Adhesions can develop between organs, tissues, or surfaces that are not normally connected, leading to organs or tissues sticking together or becoming tethered.
(c) Adhesions secondary to infection
Adhesions that occur as a secondary result of infection are fibrous bands or scar tissue that can form in the abdominal or pelvic cavity as a consequence of an infectious process. Infections, particularly those involving the abdominal or pelvic organs, can cause tissue inflammation, damage, and healing responses that may result in the formation of adhesions.
When an infection occurs, the body’s immune system responds by triggering an inflammatory response to fight off the infection. This inflammation can cause damage to tissues and organs, resulting in tissue trauma and healing responses that may involve the deposition of collagen, a fibrous protein, to promote tissue repair. However, in some cases, the healing process can result in the formation of excessive scar tissue or adhesions, leading to organs or tissues sticking together or becoming tethered.
(d) Adhesions secondary to innate pathology
Adhesions that occur as a secondary result of innate pathology refer to fibrous bands or scar tissue that form in the abdominal or pelvic cavity due to inherent or intrinsic factors within the body. Innate pathology refers to internal conditions or factors that are present in the body, often congenital or acquired, and may contribute to the development of adhesions.
There are various innate pathologies that can lead to adhesion formation. For example, certain genetic or hereditary conditions may result in abnormalities in tissue structure or function, making them more prone to forming adhesions. Conditions such as Ehlers-Danlos syndrome, Marfan syndrome, or other connective tissue disorders can affect the strength and integrity of tissues, making them more susceptible to adhesion formation.
Other innate pathologies that can contribute to adhesion formation include autoimmune disorders, chronic inflammation, or metabolic disorders that affect tissue healing and repair processes. For instance, conditions like Crohn’s disease or ulcerative colitis, which are inflammatory bowel diseases, can lead to chronic inflammation and tissue damage in the abdominal cavity, increasing the risk of adhesion formation.
What are the Symptoms of Adhesions?
Adhesions can cause a variety of symptoms, depending on their location, size, and extent. Common symptoms of adhesions may include:
Pain: Adhesions can cause localized or referred pain, which may be dull, aching, or sharp in nature. The pain may worsen with movement or certain activities, and may be persistent or intermittent.
Restricted movement: Adhesions can limit the normal movement of organs or tissues in the body, leading to restricted mobility or functional impairments. For example, adhesions in the abdominal or pelvic cavity can cause organs to become “stuck” together, resulting in restricted movement and discomfort.
Digestive symptoms: Adhesions involving the gastrointestinal tract, such as the small or large intestine, may cause symptoms such as bloating, constipation, diarrhea, nausea, or vomiting. Adhesions can also lead to bowel obstruction, which can cause severe abdominal pain, distention, and changes in bowel movements.
Gynecological symptoms: Adhesions related to gynecological conditions, such as endometriosis, can cause symptoms such as pelvic pain, painful menstrual periods, pain during sexual intercourse, and infertility.
Urinary symptoms: Adhesions involving the urinary tract, such as the bladder or ureters, may cause symptoms such as pain or discomfort during urination, frequent urination, urgency, or difficulty emptying the bladder completely.
Complications with surgery or medical procedures: Adhesions can cause complications with subsequent surgeries or medical procedures, such as difficulty in accessing the affected area, increased risk of injury or damage to surrounding organs or tissues, or decreased surgical success rates.
Other symptoms: Adhesions can also cause non-specific symptoms such as fatigue, general discomfort, or changes in body sensations.
It’s important to note that adhesions can be asymptomatic in some cases and may not cause any noticeable symptoms. However, if adhesions are suspected or if they are causing significant symptoms or functional impairments, medical evaluation and management may be needed.
What are the Common Locations of Endometriosis?
Endometriosis adhesions commonly form in the pelvic and abdominal cavity, as endometriosis is a gynecological condition where the tissue that normally lines the uterus (endometrium) grows outside of the uterus. The misplaced endometrial tissue can adhere to nearby organs or tissues, leading to the formation of adhesions.
Some common locations where endometriosis adhesions may form include:
- Ovaries: Endometriosis can cause adhesions to form between the ovaries and nearby structures such as the fallopian tubes, uterus, or pelvic sidewalls.
- Uterus: Adhesions may form between the uterus and other pelvic organs, such as the bladder or rectum, due to endometriosis.
- Pelvic sidewalls: Endometriosis adhesions can form along the sides of the pelvis, causing organs and tissues to adhere to each other and restrict movement.
- Cul-de-sac: The cul-de-sac, which is a small pouch located between the uterus and rectum, can be a common site for endometriosis adhesions to develop.
- Bowel: Endometriosis adhesions can affect the intestines, leading to adhesions between the bowel loops or between the bowel and other pelvic structures.
- Bladder: Adhesions may form between the bladder and other pelvic organs or tissues, resulting in bladder-related symptoms in cases of endometriosis.
It’s important to note that having one or more risk factors does not necessarily mean that a woman will develop fibroids, and many women with fibroids have no identifiable risk factors. The development of fibroids is likely influenced by a combination of multiple factors, and further research is needed to fully understand the complex mechanisms involved in fibroid development.
How are Adhesions Diagnosed?
Diagnosing adhesions typically involves a comprehensive evaluation by a healthcare professional, such as a gynecologist, general surgeon, or radiologist. Medical history, physical examination, and imaging studies such as ultrasound, MRI, or CT scan may be used to identify the presence of adhesions.
In some cases, diagnostic laparoscopy, a minimally invasive surgical procedure, may be performed to directly visualize and assess the extent of adhesions. During laparoscopy, the surgeon can use specialized instruments to carefully inspect the pelvic and abdominal cavity, identify adhesions, and may also perform adhesion release or removal as part of the diagnostic or therapeutic procedure.
Proper diagnosis of adhesions is important for determining appropriate treatment strategies and managing associated symptoms.
Treatment for Pelvic and Abdominal Adhesions?
The treatment of adhesions depends on various factors such as the location, extent, and severity of the adhesions, as well as the presence of symptoms and the underlying condition causing the adhesions. Here are some common surgical methods for adhesions:
Laparoscopic Surgery (Adhesiolysis)
Laparoscopic adhesion surgery, also known as adhesiolysis, is a minimally invasive surgical procedure that is commonly used to treat adhesions in the pelvic and abdominal cavity. During laparoscopic adhesion surgery, small incisions are made in the abdominal wall, and a laparoscope (a thin, flexible tube with a light and camera) is inserted to visualize the adhesions. Specialized instruments are then used to carefully separate and release the adhesions, allowing the affected organs and tissues to move more freely.
Laparoscopic adhesion surgery offers several advantages over open surgery, including smaller incisions, less postoperative pain, shorter hospital stays, and quicker recovery times. However, it is a technically challenging procedure that requires expertise in laparoscopic techniques, and not all adhesions can be safely and effectively treated laparoscopically, depending on the location, extent, and severity of the adhesions.
After laparoscopic adhesion surgery, additional measures such as adhesion barriers may be used to reduce the risk of adhesions re-forming. Postoperative care typically includes pain management, wound care, and a gradual return to normal activities under the guidance of the surgical team.
Robotic-Assisted Adhesiolysis
Robotic surgery is a minimally invasive surgical approach that uses specialized robotic-assisted surgical systems to perform complex surgical procedures with enhanced precision and control. Robotic surgery has been used in various surgical specialties, including gynecological surgery for the treatment of adhesions.
In the context of adhesion surgery, robotic-assisted techniques can be utilized for adhesiolysis, which is the surgical removal or division of adhesions that have formed in the pelvic or abdominal cavity. Robotic adhesiolysis typically involves the use of a surgical robot, such as the da Vinci Surgical System, which provides the surgeon with enhanced dexterity and visualization, allowing for precise and meticulous dissection of adhesions.
The benefits of robotic adhesiolysis may include reduced postoperative pain, shorter hospital stays, faster recovery, and improved cosmetic outcomes compared to traditional open surgery. However, it’s important to note that the availability and use of robotic surgery, including for adhesion treatment, may vary depending on the healthcare facility, surgeon’s experience and expertise, and individual patient factors.
Adhesions Barrier
Adhesion barriers are medical devices used during surgery to help reduce the formation of adhesions, which are abnormal bands of scar tissue that can form between tissues or organs after surgery or injury. Adhesion barriers work by creating a physical barrier between tissues or organs, preventing them from sticking together during the healing process.
Adhesion barriers may be made of different materials, such as synthetic polymers, collagen, or hyaluronic acid, and may come in the form of sheets, gels, or sprays.
The use of adhesion barriers can help reduce the risk of adhesion formation and potentially decrease the complications associated with adhesions, such as pain, bowel obstruction, and infertility. However, it’s important to note that not all surgical procedures require or benefit from the use of adhesion barriers, and their use should be determined on a case-by-case basis by the surgeon based on the patient’s individual circumstances and the specific surgical procedure being performed.
Service Areas
NYGSE provides specialized care for pelvic adhesions to women throughout Babylon and Bay Shore, NY, focusing on careful evaluation and minimally invasive treatment approaches tailored to each patient’s condition.
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Have Questions About Your Surgery or Treatment?
Expert treatment. Compassionate care. Real results.
November 18, 2025by admin
Levator Ani Syndrome
What Is Levator Ani Syndrome?
Levator Ani Syndrome is a chronic pelvic floor disorder in which the levator ani muscles—responsible for supporting the bladder, uterus, and rectum—become overly tense, irritated, or spasmed. This can produce persistent pressure, burning, or deep aching in the pelvis, rectum, or lower abdomen. Symptoms often worsen with prolonged sitting, bowel movements, or sexual activity. While the exact cause varies, factors such as muscle tension, nerve irritation, prior pelvic surgery, trauma, and endometriosis are all known to contribute.
Medical illustration showing the levator ani muscles within the pelvic floor, highlighting key components—including the pubococcygeus, iliococcygeus, and puborectalis—that support the pelvic organs. Used to demonstrate how muscle tension or irritation in this area can lead to chronic pelvic pain.
COMMON QUESTIONS ABOUT Levator Ani Syndrome
Causes of Sciatic Endometriosis
The exact cause of sciatic endometriosis is not yet fully understood, but it is believed to occur when endometrial tissue grows outside the uterus and attaches to or infiltrates the sciatic nerve.
Endometrial tissue can grow in different areas of the body due to a process called retrograde menstruation. During menstruation, some endometrial tissue flows backwards through the fallopian tubes and into the pelvic cavity instead of being expelled from the body. This misplaced tissue can then implant and grow on organs and tissues outside of the uterus, including the sciatic nerve.
Other factors that may contribute to the development of sciatic endometriosis include genetics, hormonal imbalances, immune system dysfunction, and environmental toxins.
Risk factors for endometriosis, such as a family history of the condition, early onset of menstrual periods, and prolonged menstrual cycles, may also increase the risk of developing sciatic endometriosis.
If sciatic endometriosis is the underlying cause of the sciatica, leg pain may emerge or worsen just before or during menstrual periods. This is because endometriosis is linked to hormonal changes, and as estrogen and progesterone fluctuate during the menstrual cycle, they can trigger pain in the legs.
Causes of Sciatic Endometriosis
The exact cause of sciatic endometriosis is not yet fully understood, but it is believed to occur when endometrial tissue grows outside the uterus and attaches to or infiltrates the sciatic nerve.
Endometrial tissue can grow in different areas of the body due to a process called retrograde menstruation. During menstruation, some endometrial tissue flows backwards through the fallopian tubes and into the pelvic cavity instead of being expelled from the body. This misplaced tissue can then implant and grow on organs and tissues outside of the uterus, including the sciatic nerve.
Other factors that may contribute to the development of sciatic endometriosis include genetics, hormonal imbalances, immune system dysfunction, and environmental toxins.
Risk factors for endometriosis, such as a family history of the condition, early onset of menstrual periods, and prolonged menstrual cycles, may also increase the risk of developing sciatic endometriosis.
If sciatic endometriosis is the underlying cause of the sciatica, leg pain may emerge or worsen just before or during menstrual periods. This is because endometriosis is linked to hormonal changes, and as estrogen and progesterone fluctuate during the menstrual cycle, they can trigger pain in the legs.
Diagnosis of Sciatic Endometriosis
Sciatic endometriosis can be challenging to diagnose since it typically mimics the symptoms of sciatica. Nonetheless, it usually occurs alongside regular endometriosis. If a woman has already been diagnosed with endometriosis and experiences sciatica symptoms, sciatic endometriosis may be suspected. Imaging techniques such as magnetic electromyography, computed tomography (CT) scan, magnetic resonance imaging (MRI), or surgery may be used to diagnose the condition.
Additionally, a test called Lasègue’s test or straight leg raise test can provide an indication of sciatic endometriosis. During the test, the patient lies on her back, and the doctor raises the patient’s legs with the knees kept straight. If the sciatic nerve is under pressure due to sciatic endometriosis, the patient will experience sciatic pain when the legs reach an angle of 30 to 70 degrees relative to the examination table.
Early diagnosis is crucial since sciatic endometriosis can result in irreversible nerve damage caused by recurrent bleeding and scarring if left untreated.
Treatment for Levator Ani Syndrome
Surgical intervention is generally not considered as a first-line treatment for Levator Ani Syndrome, as it is primarily a functional disorder of the pelvic floor muscles. However, in some cases where conservative treatments have failed to provide relief, or if there are specific underlying anatomical abnormalities that contribute to the condition, surgical methods may be considered as a treatment option.
The surgical treatment options for Levator Ani Syndrome may include:
Trigger Point Injections
Levator Ani Syndrome trigger point injections are a procedure that involves injecting a local anesthetic, such as lidocaine, into the trigger points in the levator ani muscles, which are localized areas of hyper-irritable muscles. The goal of trigger point injections is to provide temporary relief from muscle tension and pain associated with Levator Ani Syndrome.
The trigger point injections are typically performed by a qualified healthcare professional, such as a gynecologist, urologist, or pain management specialist. The procedure is usually done in an outpatient setting, and the patient may be positioned in a specific way, such as in a lithotomy position, which is similar to the position used during a gynecological exam.
During the procedure, the healthcare provider will use a thin needle to inject a small amount of local anesthetic into the trigger points in the levator ani muscles, which are identified based on the patient’s symptoms and physical examination. The local anesthetic helps to numb the trigger points and temporarily relax the muscles, providing relief from pain and muscle tension.
Trigger point injections for Levator Ani Syndrome are typically performed as part of a comprehensive treatment plan that may also include other conservative measures, such as pelvic floor physical therapy, medication, and lifestyle modifications. The effectiveness of trigger point injections can vary among individuals, and the relief may be temporary. Repeat injections may be needed depending on the individual’s response to the treatment. The decision to undergo trigger point injections should be made in consultation with a qualified healthcare professional, taking into account the individual’s specific condition and overall health.
It’s recommended to request an appointment with New York Gynecology Endometriosis (NYGE) to obtain an accurate estimate of the cost.
Muscle Release Surgery
Muscle release surgery may be considered as a treatment option for Levator Ani Syndrome in cases where conservative measures, such as physical therapy, medications, and trigger point injections, have not provided adequate relief.
The goal of muscle release surgery for Levator Ani Syndrome is to release or alleviate the tension, tightness, or contracture in the levator ani muscles, which can be contributing to the pain and discomfort associated with the condition. The surgical procedure typically involves cutting or releasing the affected muscle fibers or fascia to improve muscle function and reduce pain.
The specific approach and technique used in muscle release surgery for Levator Ani Syndrome may vary depending on the severity and location of the condition. This may include techniques such as myotomy, myofascial release, or tenotomy, depending on the specific needs of the individual patient.
It’s important to note that muscle release surgery for Levator Ani Syndrome is typically considered as a last resort when other conservative treatments have not been effective, and the decision to undergo surgery should be made in consultation with a qualified healthcare provider such as New York Gynecology Endometriosis (NYGE).
Biofeedback
Levator ani biofeedback is a therapeutic technique used to treat Levator Ani Syndrome, which is a condition characterized by chronic pelvic pain caused by tension or dysfunction of the levator ani muscles. Biofeedback is a non-invasive treatment approach that aims to help individuals gain conscious control over the levator ani muscles by providing them with real-time feedback on their muscle activity.
During a levator ani biofeedback session, sensors or electrodes are placed on or near the levator ani muscles to measure their activity. The information is then relayed to the individual through visual or auditory feedback, allowing them to see or hear their muscle activity in real-time. The individual can then learn to modulate their muscle activity based on the feedback provided, with the goal of improving muscle coordination, relaxation, and function.
Service Areas
NYGSE provides specialized care for women throughout Babylon and Bay Shore, NY dealing with levator ani syndrome, focusing on accurate diagnosis and tailored treatment strategies to reduce chronic pelvic discomfort and improve daily function.
References
Anatomy, abdomen and pelvis: Levator ani muscle. (October 26, 2022). National Library of Medicine – National Center for Biotechnology Information. https://www.ncbi.nlm.nih.gov/books/NBK556078/
Aredo JV, Heyrana KJ, Karp BI, Shah JP, Stratton P. Relating chronic pelvic pain and endometriosis to signs of sensitization and myofascial pain and dysfunction. National Library of Medicine – National Center for Biotechnology Information. doi: 10.1055/s-0036-1597123
Azzam, H., Halim, M., El-Assaly, H. et al. MRI comparative study of levator ani muscle changes in nulliparous and multiparous females. Egypt J Radiol Nucl Med 50, 56 (2019). https://doi.org/10.1186/s43055-019-0065-0
Biofeedback for somatic conditions. (2022). Johns Hopkins Medicine – Johns Hopkins Healthcare. https://hpo.johnshopkins.edu/doc/fetch.cfm/iQbkLDA2
Christopher R. Chapple (2006). Multidisciplinary management of female pelvic floor disorders. Churchill Livingstone. pp. 4–. ISBN 978-0-443-07272-7
The levator ani (pelvic diaphragm). Copyright 2011 by Lawrence Rizzolo and William Stewart, Yale School of Medicine. http://anatomy.medicine.yale.edu/VisibleHumanLessonPlans/LevatorAni.htm
Tomashev, R., Abbas Shobeiri, S. The levator ani muscle repair: a call to action. Tech Coloproctol 25, 897–899 (2021). https://doi.org/10.1007/s10151-021-02480-1
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Have Questions About Your Surgery or Treatment?
Expert treatment. Compassionate care. Real results.
November 18, 2025by admin
Sciatic Endometriosis
What Is Sciatic Endometriosis?
Sciatic endometriosis is a rare but extremely painful form of endometriosis in which endometrial-like tissue grows on or around the sciatic nerve—the largest nerve in the body. Because the sciatic nerve runs from the lower spine through the pelvis and down each leg, even a small lesion can trigger severe nerve irritation. For many patients, symptoms flare or worsen during menstruation, making the condition easy to mistake for orthopedic sciatica. Without early diagnosis and intervention, sciatic endometriosis can lead to chronic nerve damage, weakness, and mobility challenges.
Illustration showing the sciatic nerve running from the lower spine through the pelvis and down the leg, with a highlighted region indicating nerve irritation. Used to demonstrate how endometriosis affecting the sciatic nerve can cause radiating leg, hip, and pelvic pain.
COMMON QUESTIONS ABOUT Sciatic Endometriosis
What are the Causes of Sciatic Endometriosis?
The exact cause of sciatic endometriosis is not yet fully understood, but it is believed to occur when endometrial tissue grows outside the uterus and attaches to or infiltrates the sciatic nerve.
Endometrial tissue can grow in different areas of the body due to a process called retrograde menstruation. During menstruation, some endometrial tissue flows backwards through the fallopian tubes and into the pelvic cavity instead of being expelled from the body. This misplaced tissue can then implant and grow on organs and tissues outside of the uterus, including the sciatic nerve.
Other factors that may contribute to the development of sciatic endometriosis include genetics, hormonal imbalances, immune system dysfunction, and environmental toxins.
Risk factors for endometriosis, such as a family history of the condition, early onset of menstrual periods, and prolonged menstrual cycles, may also increase the risk of developing sciatic endometriosis.
If sciatic endometriosis is the underlying cause of the sciatica, leg pain may emerge or worsen just before or during menstrual periods. This is because endometriosis is linked to hormonal changes, and as estrogen and progesterone fluctuate during the menstrual cycle, they can trigger pain in the legs.
How is Sciatic Endometriosis Diagnosed?
Sciatic endometriosis can be challenging to diagnose since it typically mimics the symptoms of sciatica. Nonetheless, it usually occurs alongside regular endometriosis. If a woman has already been diagnosed with endometriosis and experiences sciatica symptoms, sciatic endometriosis may be suspected. Imaging techniques such as magnetic electromyography, computed tomography (CT) scan, magnetic resonance imaging (MRI), or surgery may be used to diagnose the condition.
Additionally, a test called Lasègue’s test or straight leg raise test can provide an indication of sciatic endometriosis. During the test, the patient lies on her back, and the doctor raises the patient’s legs with the knees kept straight. If the sciatic nerve is under pressure due to sciatic endometriosis, the patient will experience sciatic pain when the legs reach an angle of 30 to 70 degrees relative to the examination table.
Early diagnosis is crucial since sciatic endometriosis can result in irreversible nerve damage caused by recurrent bleeding and scarring if left untreated.
Surgical Methods for the Treatment of Sciatic Endometriosis
The most effective treatment for sciatic endometriosis is surgical removal of the endometrial tissue that is compressing the sciatic nerve. Surgery can also help to address any scarring or adhesions that may have formed due to the condition.
Laparoscopic Surgery
Laparoscopic surgery is a minimally invasive surgical technique that may be used to remove endometrial tissue causing sciatic endometriosis. The procedure involves making small incisions in the abdomen through which a tiny camera and surgical instruments are inserted.
During laparoscopic surgery for sciatic endometriosis, the surgeon will locate and remove the endometrial lesions causing pressure on the sciatic nerve. This may involve removing small pieces of tissue or larger, more extensive areas of endometriosis.
One advantage of laparoscopic surgery is that it typically results in less pain and scarring than open surgery. It also typically has a shorter recovery time, with most patients able to return to their normal activities within a few days to a week.
However, laparoscopic surgery may not be appropriate for all cases of sciatic endometriosis, particularly in cases where the endometrial lesions are extensive or in difficult-to-reach areas. In such cases, open surgery may be necessary to remove the affected tissue. The choice of surgical approach will depend on the individual case and the judgment of the treating physician.
Open Surgical Approach
Open surgical approaches to treating sciatic endometriosis involve making a larger incision in the abdomen or pelvis to access the affected area. This technique is typically reserved for cases where laparoscopic or robotic-assisted surgery is not feasible or safe.
During open surgery, the surgeon may remove the affected tissue, scar tissue, and endometrial lesions from around the sciatic nerve. The procedure may also involve repairing any damage to the nerve itself, such as removing any constrictions or freeing it from any adhesions.
Open surgical approaches for sciatic endometriosis can be more invasive than laparoscopic or robotic-assisted surgery and may require a longer hospital stay and recovery time. Additionally, open surgery can result in more scarring and pain than the less invasive approaches. However, in some cases, open surgery may be the best option for treating severe or complicated cases of sciatic endometriosis.
The cost of open surgical approaches for sciatic endometriosis can vary depending on several factors such as the location of the medical facility, the surgeon’s fees, and any additional charges associated with the procedure. It is important for patients to discuss the potential costs and any insurance coverage or payment options with New York Gynecology Surgery & Endometriosis (NYGSE) and insurance provider.
Robotic-Assisted Laparoscopic Surgery
Robotic-assisted laparoscopic surgery is a minimally invasive surgical technique that uses a robotic system to aid in performing the procedure. The robotic system consists of a console operated by the surgeon, which controls the robotic arms that hold the surgical instruments. This allows for greater precision and dexterity during the surgery.
Robotic-assisted laparoscopic surgery for sciatic endometriosis is a newer and less commonly used technique compared to traditional laparoscopic surgery. The cost of this procedure can vary depending on several factors such as the location of the medical facility, the surgeon’s fees, and any additional charges associated with the use of the robotic system.
As with any medical procedure, it is important for patients to check with their insurance provider and the treating physician to determine the expected cost of the procedure and any potential out-of-pocket expenses they may incur. It is also important to discuss any potential financial assistance or payment options that may be available.
Service Areas
NYGSE provides expert care for women throughout Babylon and Bay Shore, NY with sciatic endometriosis, focusing on complex cases involving nerve pathways and delivering precise, individualized treatment close to home.
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Have Questions About Your Surgery or Treatment?
Expert treatment. Compassionate care. Real results.
November 18, 2025by admin
Frozen Pelvis
What Is a Frozen Pelvis in Endometriosis?
A frozen pelvis describes an advanced, severe form of endometriosis in which pelvic organs become so densely bound together by adhesions that their normal movement is almost completely lost. Although not an official medical diagnosis, the term is widely used to describe the extreme immobility, distortion, and anatomical fixation caused by deeply infiltrating endometriosis. In this state, organs such as the uterus, ovaries, bowel, bladder, ureters, and pelvic ligaments become fused together by thick fibrotic tissue, often resulting in severe pain, impaired function, and complex surgical challenges.
This laparoscopic image shows a frozen pelvis caused by extensive deep infiltrating endometriosis. Multiple pelvic organs—including the ovaries, rectum, and surrounding peritoneal tissue—are tightly adhered by dense, fibrotic adhesions, creating severe immobility and distorted anatomy. This presentation is typical of advanced-stage endometriosis where chronic inflammation leads to scarring, organ fixation, and loss of normal pelvic separation.
COMMON QUESTIONS ABOUT Frozen Pelvis in Endometriosis
How Common is Frozen Pelvis in Endometriosis?
The exact prevalence of frozen pelvis in endometriosis is challenging to determine due to variations in diagnostic criteria, study populations, and methodologies. However, frozen pelvis is considered a relatively uncommon but severe complication of endometriosis. It occurs when the pelvic organs become densely adhered to each other due to extensive endometriotic involvement and the formation of scar tissue (adhesions).
Frozen pelvis is more commonly observed in advanced stages of endometriosis, particularly when deeply infiltrating endometriosis (DIE) affects the pelvic organs such as the rectum, bladder, uterus, and bowel. It can also involve the fallopian tubes, ovaries, and pelvic ligaments.
While specific prevalence rates are lacking, estimates suggest that frozen pelvis occurs in a minority of individuals with endometriosis, ranging from around 5% to 15% of cases. It is important to note that these numbers may vary based on the population studied and the diagnostic criteria used.
Early detection and appropriate management of endometriosis are crucial to minimize the risk of developing a frozen pelvis. Regular medical follow-up, effective pain management, and timely intervention can help prevent the progression of endometriosis to severe adhesions and frozen pelvis.
What are the Symptoms of Frozen Pelvis?
The symptoms of frozen pelvis can vary depending on the underlying cause and the specific organs involved. However, common symptoms associated with frozen pelvis include:
- Chronic pelvic pain: Persistent and severe pain in the pelvic region is a hallmark symptom of frozen pelvis. The pain may be dull, aching, or sharp in nature and can be constant or intermittent.
- Limited mobility: Frozen pelvis can result in restricted movement and reduced flexibility in the pelvic area. This can lead to difficulty in bending, twisting, or performing normal daily activities.
- Pain during sexual intercourse: Adhesions and organ fixation in the pelvis can cause pain and discomfort during sexual intercourse, known as dyspareunia.
- Bowel and bladder dysfunction: Adhesions involving the bowel and bladder can lead to symptoms such as constipation, diarrhea, bloating, urinary urgency, or difficulty emptying the bladder.
- Infertility or reproductive issues: In some cases, frozen pelvis can impact fertility by obstructing or distorting the fallopian tubes, affecting egg release, or impairing implantation.
- Gastrointestinal symptoms: Depending on the extent and location of adhesions, symptoms like abdominal pain, bloating, nausea, and changes in bowel habits may be present.
It’s important to note that these symptoms are not exclusive to frozen pelvis and can be associated with other pelvic conditions as well. If you are experiencing any of these symptoms, it is advisable to request an appointment with New York Gynecology Endometriosis (NYGE) for a comprehensive evaluation and appropriate diagnosis.
How is Frozen Pelvis Classified?
This classification provides additional information about the location and distribution of adhesions within the pelvis. The most commonly used classification based on patterns is the American Society for Reproductive Medicine (ASRM) classification. The ASRM classification system divides frozen pelvis into four patterns:
- Pattern I (Uterosacral ligament involvement): This pattern involves adhesions primarily affecting the uterosacral ligaments, which are fibrous bands that attach the uterus to the sacrum (the triangular bone at the base of the spine). Adhesions in this pattern can cause fixation of the uterus and limited mobility of the pelvic structures.
- Pattern II (Posterior cul-de-sac involvement): In this pattern, adhesions primarily involve the posterior cul-de-sac, also known as the Pouch of Douglas. The cul-de-sac is the space between the uterus and rectum. Adhesions in this pattern can lead to the uterus and other pelvic structures being fixed in a posterior position.
- Pattern III (Anterior cul-de-sac involvement): This pattern involves adhesions primarily affecting the anterior cul-de-sac, which is the space between the uterus and bladder. Adhesions in this pattern can cause fixation of the uterus and other pelvic structures in an anterior position.
- Pattern IV (Diffuse involvement): In this pattern, adhesions are widespread and involve multiple areas of the pelvis, including the uterosacral ligaments, posterior cul-de-sac, and anterior cul-de-sac. The adhesions in this pattern are often dense and can cause significant distortion and fixation of pelvic structures.
The pattern classification provides information about the specific areas affected by adhesions and can help guide surgical planning and treatment approaches. It assists in determining the complexity of the frozen pelvis and the potential challenges that may be encountered during surgical intervention. However, it’s important to note that the patterns may overlap or coexist in some cases, and individual variations can exist within each pattern.
Which healthcare professionals are qualified to perform surgery for a frozen pelvis?
Surgery for a frozen pelvis should ideally be performed by a skilled and experienced surgical team that includes healthcare professionals with expertise in the management of endometriosis and complex pelvic conditions. The specific specialists involved may vary depending on the extent and nature of the frozen pelvis, as well as the individual patient’s needs. Here are some healthcare professionals who may be involved in the surgical management of a frozen pelvis:
- Gynecologist: Gynecologists with advanced training and experience in the surgical treatment of endometriosis are often the primary surgeons involved in addressing a frozen pelvis. They specialize in the diagnosis and management of conditions affecting the female reproductive system, including endometriosis.
- Colorectal surgeon: If the frozen pelvis involves significant bowel involvement or adhesions, a colorectal surgeon may be consulted or directly involved in the surgical procedure. They specialize in the diagnosis and treatment of conditions affecting the colon, rectum, and anus.
- Urologist: In cases where the frozen pelvis affects the bladder, ureters, or other urinary structures, a urologist may be involved in the surgical management. Urologists specialize in the diagnosis and treatment of urinary system disorders.
- Multidisciplinary team: Depending on the complexity of the frozen pelvis and associated conditions, a multidisciplinary team may be formed, involving gynecologists, colorectal surgeons, urologists, and other specialists. This collaborative approach ensures comprehensive evaluation, surgical planning, and coordinated care.
It is crucial to seek treatment from healthcare professionals or medical centers like New York Gynecology Endometriosis (NYGE) with experience in managing frozen pelvis and the associated conditions. They can provide an accurate diagnosis, evaluate the extent of the condition, and recommend appropriate surgical interventions based on individual circumstances.
Surgical Treatment of Frozen Pelvis Causes by Endometriosis
The surgical treatment of frozen pelvis caused by endometriosis typically involves a comprehensive approach aimed at relieving adhesions, restoring normal pelvic anatomy and function, and alleviating associated symptoms. The specific surgical procedures performed may vary depending on the extent and severity of the adhesions and the individual patient’s circumstances.
Here are some common surgical treatment options:
Laparoscopic surgery
Laparoscopy is a minimally invasive surgical technique commonly used for the treatment of endometriosis-related frozen pelvis. It involves making small incisions in the abdomen through which a thin, flexible camera (laparoscope) and surgical instruments are inserted. The surgeon can visualize the pelvic organs and carefully dissect and remove the adhesions.
According to the Healthcare Bluebook, the cost of laparoscopic excision surgery ranges from $6,440 to $20,380, with an average cost of $13,790 in the United States. However, it’s important to note that the actual cost may vary depending on several factors such as the location of the facility, the experience of the surgeon, and the complexity of the procedure. It’s also worth checking with your insurance provider to see what portion of the cost will be covered.
To obtain an accurate cost estimate, it is advisable to make an appointment with New York Gynecology Surgery & Endometriosis (NYGSE).
Adhesiolysis
Adhesiolysis refers to the surgical removal or separation of adhesions. During this procedure, the surgeon carefully separates the adhered organs, restoring their mobility and function. Various techniques, such as sharp dissection, electrocautery, or laser therapy, may be utilized to release the adhesions.
Excision of Endometriosis Lesions
If endometriosis lesions are present within the adhesions, the surgeon may perform excision or removal of these abnormal growths. Excision aims to completely remove the endometriotic tissue while preserving the healthy surrounding tissue.
Organ-specific Procedures
In cases where specific pelvic organs, such as the bowel, bladder, ureters, or uterus, are significantly involved in the frozen pelvis, additional procedures may be required. These may include bowel resection or re-anastomosis, bladder repair, ureteral re-implantation, or even hysterectomy (removal of the uterus) if necessary.
Multidisciplinary Approach
Depending on the complexity of the frozen pelvis and associated symptoms, a multidisciplinary approach involving gynecologists, colorectal surgeons, urologists, or other specialists may be required to optimize surgical outcomes.
Service Areas
NYGSE provides expert treatment for women throughout Babylon and Bay Shore, NY living with frozen pelvis, focusing on restoring mobility of affected organs through precise, individualized surgical planning.
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Have Questions About Your Surgery or Treatment?
Expert treatment. Compassionate care. Real results.
November 18, 2025by admin
Deep Infiltrating Endometriosis (DIE)
Deep Infiltrating Endometriosis (DIE)
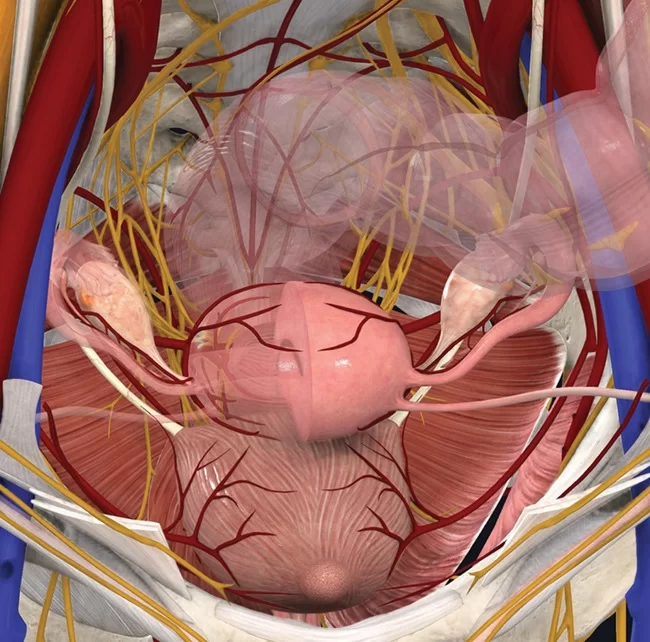
Deep infiltrating endometriosis (DIE) is one of the most severe forms of endometriosis, defined by lesions that penetrate several millimeters or more into surrounding organs and tissues. Unlike superficial disease, DIE often involves critical structures such as the bowel, bladder, ureters, uterosacral ligaments, and pelvic nerves. Because these lesions trigger chronic inflammation, scarring, adhesions, and sometimes organ dysfunction, DIE is frequently associated with severe pain, gastrointestinal or urinary symptoms, and infertility. Accurate diagnosis and treatment require evaluation by specialists experienced in advanced endometriosis care.
Illustration showing endometrial implants affecting the ovaries, fallopian tubes, and pelvic structures. Deep infiltrating endometriosis extends beyond superficial surfaces and can invade vital tissues, contributing to pain, inflammation, and organ dysfunction.
COMMON QUESTIONS ABOUT DEEP Infiltrating Endometriosis
Why Deep Infiltrating Endometriosis Is More Invasive?
Deep infiltrating endometriosis (DIE) is considered a highly invasive form of endometriosis due to its ability to penetrate deeply into the surrounding tissues and organs. It is characterized by the growth of endometrial tissue outside the uterus, typically in the pelvic region, but can also affect other areas of the body.
Endometriosis itself is a condition in which the tissue that normally lines the uterus (endometrium) grows outside of it. In the case of deep infiltrating endometriosis, this misplaced endometrial tissue infiltrates and implants into the surrounding structures, such as the pelvic cavity, ovaries, fallopian tubes, bladder, and bowel.
Several factors contribute to the invasiveness of deep infiltrating endometriosis:
Depth of infiltration: Unlike superficial endometriosis, which affects the outermost layers of tissue, deep infiltrating endometriosis infiltrates deeply into the tissues and organs. It can penetrate several millimeters or even centimeters beneath the surface, leading to significant involvement and adhesion formation.
Invasion of surrounding structures: Deep infiltrating endometriosis can invade nearby organs and tissues, such as the bowel or bladder. The abnormal growth of endometrial tissue can cause adhesions, scarring, and structural changes in these organs, leading to pain, inflammation, and other symptoms.
Inflammatory response: The presence of endometrial tissue outside the uterus triggers an inflammatory response in the affected areas. Chronic inflammation can lead to tissue damage, fibrosis, and further invasion of surrounding tissues.
Nerve involvement: Deep infiltrating endometriosis can affect nerves in the pelvic region, leading to severe pain and discomfort. The infiltrating tissue can irritate or compress the nerves, causing persistent pain even in the absence of menstrual bleeding.
What are the Causes of Deep Infiltrating Endometriosis?
The exact causes of Deep Infiltrating Endometriosis (DIE) are not fully understood, but there are several theories that help explain its development.
One prominent theory is retrograde menstruation, which suggests that during menstruation, menstrual blood containing endometrial cells flows backward through the fallopian tubes into the pelvic cavity instead of exiting the body. These displaced endometrial cells can then implant and grow on the pelvic organs, leading to the development of endometriosis, including the deep infiltrating form. However, retrograde menstruation alone cannot fully explain the occurrence of DIE, as many women experience retrograde menstruation without developing the condition.
Other contributing factors may include hormonal imbalances, genetic predisposition, impaired immune system function, and environmental factors. Hormones such as estrogen are known to stimulate the growth of endometrial tissue. Therefore, hormonal imbalances or abnormalities could promote the development and progression of endometriosis. Genetic factors may also play a role, as endometriosis tends to run in families, suggesting a hereditary component. Additionally, certain environmental factors, such as exposure to toxins or chemicals, could potentially influence the development of endometriosis, although more research is needed to establish a definitive link.
It’s important to note that while these theories provide some insight into the potential causes of deep infiltrating endometriosis, the condition likely results from a combination of multiple factors rather than a single cause. Further research is still needed to fully understand the complex origins of DIE.
What are the Symptoms of Deep Infiltrating Endometriosis?
Deep Infiltrating Endometriosis (DIE) is associated with a range of symptoms that can significantly impact a person’s quality of life. These symptoms often vary in severity and can include:
- Chronic pelvic pain: Persistent and debilitating pain in the pelvic region is a common symptom of DIE. The pain may worsen during menstruation, sexual intercourse (dyspareunia), or bowel movements. It can also be present throughout the menstrual cycle and may extend to the lower back and thighs.
- Gastrointestinal disturbances: Deep infiltrating endometriosis can affect the gastrointestinal tract, leading to symptoms such as bloating, diarrhea, constipation, nausea, and abdominal cramps. Some individuals may also experience rectal bleeding or pain during bowel movements.
- Urinary symptoms: DIE can involve the urinary system, resulting in symptoms like frequent urination, urgency, pain during urination, or blood in the urine.
- Infertility: Deep infiltrating endometriosis is associated with fertility problems. The abnormal growth and scarring caused by endometriosis can obstruct the fallopian tubes or affect the quality of the eggs or sperm, making it more difficult to conceive.
- Painful intercourse: Deep infiltrating endometriosis can cause deep pelvic pain during sexual intercourse, which is known as dyspareunia.
It is important to remember that the severity and presentation of symptoms can vary widely among individuals, and some may experience no symptoms at all. Scheduling an appointment with New York Gynecology Surgery & Endometriosis (NYGSE) is crucial for an accurate diagnosis and appropriate management of deep infiltrating endometriosis.
Is Deep Infiltrating Endometriosis life threatening?
Deep Infiltrating Endometriosis (DIE) itself is not typically considered life-threatening. However, it can significantly impact a person’s quality of life and cause chronic pain and other symptoms that can be debilitating. The severity of symptoms can vary among individuals, and some may experience more severe complications related to DIE.
While DIE itself is not life-threatening, complications arising from the condition can have serious implications. For example, if endometriosis infiltrates the bowel, it can lead to bowel obstruction or perforation, requiring medical intervention. In rare cases, extensive DIE involvement in vital organs or structures can cause severe complications, but such instances are uncommon.
It’s important for individuals with deep infiltrating endometriosis to receive appropriate medical care and management to alleviate symptoms, minimize complications, and improve their overall well-being. Regular follow-ups with healthcare providers and adherence to treatment plans can help address the impact of DIE on daily life and reproductive health.
How is Deep Infiltrating Endometriosis Diagnosed?
The diagnosis of deep infiltrating endometriosis (DIE) typically involves a combination of medical history evaluation, physical examination, imaging studies, and surgical procedures. Here is an overview of the diagnostic methods commonly used:
- Medical history and symptom assessment: The healthcare provider will gather information about your symptoms, menstrual cycle, pain patterns, and any other relevant medical history.
- Pelvic examination: A pelvic examination may be performed to check for any abnormalities, tenderness, or masses in the pelvic region.
- Imaging studies: Imaging techniques such as transvaginal ultrasound (TVUS) or pelvic MRI (magnetic resonance imaging) can help visualize the pelvic structures and detect the presence of endometrial growths or adhesions. These imaging modalities can provide valuable information about the location and extent of the endometriosis.
- Laparoscopy: Laparoscopy is a surgical procedure considered the gold standard for diagnosing endometriosis, including deep infiltrating endometriosis. It involves making small incisions in the abdomen to insert a laparoscope (a thin, lighted tube with a camera) to visualize the pelvic organs directly. During laparoscopy, the surgeon can identify and evaluate the location, size, and depth of the endometrial lesions, and may also perform biopsies for confirmation.
It’s important to note that definitive diagnosis of deep infiltrating endometriosis can only be made through surgical intervention, typically laparoscopy. Other diagnostic methods, such as imaging, can provide supportive evidence but may not offer a conclusive diagnosis.
Diagnosing deep infiltrating endometriosis requires the expertise of a gynecologist or a specialist in reproductive medicine who is experienced in evaluating and treating endometriosis.
Surgical Methods for the Treatment of Deep Infiltrating Endometriosis
The surgical treatment of deep infiltrating endometriosis (DIE) aims to remove or excise the endometrial implants, relieve symptoms, and improve the patient’s quality of life. Several surgical methods may be employed, depending on the location, extent, and severity of the endometriosis lesions.
Here are some common surgical methods used in the treatment of DIE:
Laparoscopic Excision Surgery
Laparoscopic surgery is the preferred approach for treating DIE. It involves making small incisions in the abdomen and inserting specialized surgical instruments, including a laparoscope, to visualize and access the pelvic organs. Using these instruments, the surgeon can carefully excise or remove the endometrial implants and associated scar tissue while preserving healthy tissue.
According to the Healthcare Bluebook, the cost of laparoscopic excision surgery ranges from $6,440 to $20,380, with an average cost of $13,790 in the United States. However, it’s important to note that the actual cost may vary depending on several factors such as the location of the facility, the experience of the surgeon, and the complexity of the procedure. It’s also worth checking with your insurance provider to see what portion of the cost will be covered.
To obtain an accurate cost estimate, it is advisable to make an appointment with NYGSE.
Nerve-Sparing Surgery
In cases where deep infiltrating endometriosis involves nerves, such as the pelvic nerves or sciatic nerves, nerve-sparing surgical techniques may be employed. The goal is to excise the endometrial lesions while minimizing damage to the nerves and preserving their function.
Bowel Resection or Repair
If deep infiltrating endometriosis affects the bowel, segments of the affected bowel may need to be resected (surgically removed) and reconstructed. This procedure is typically performed by a specialist, such as a colorectal surgeon, in collaboration with a gynecologist.
Bladder or Ureteral Surgery
If the endometrial implants infiltrate the bladder or the ureters (the tubes connecting the kidneys to the bladder), surgical intervention may be required to excise the lesions and restore normal urinary function. This procedure may involve collaboration between urologists and gynecologists.
Hysterectomy
In cases where other treatments have been unsuccessful, and the patient no longer desires fertility, a hysterectomy (removal of the uterus) may be considered. This procedure can be performed either laparoscopically or through an abdominal incision (laparotomy). In some cases, the removal of the ovaries (oophorectomy) may be recommended as well.
Service Areas
For women in Babylon and Bay Shore, NY facing deep infiltrating endometriosis (DIE), NYGSE offers a highly specialized level of care focused on identifying and treating disease that extends beneath the surface and affects surrounding structures.
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Have Questions About Your Surgery or Treatment?
Expert treatment. Compassionate care. Real results.
November 17, 2025by admin
Peritoneal Endometriosis
Understanding Peritoneal Endometriosis
Peritoneal endometriosis occurs when tissue similar to the uterine lining implants onto the peritoneum — the thin membrane that lines the abdominal cavity. These lesions can form on pelvic organs, the abdominal wall, and even higher structures such as the diaphragm. As these implants become inflamed or form adhesions, they can cause pelvic pain, menstrual irregularities, gastrointestinal symptoms, and infertility. Because peritoneal endometriosis ranges from subtle superficial lesions to deeply infiltrating disease, diagnosis often requires specialized evaluation and, in many cases, laparoscopic confirmation.
This illustration shows a cross-section of the upper abdomen, highlighting the greater peritoneal cavity, the lesser sac, and the surrounding ligaments. The peritoneum is the thin, protective membrane lining these spaces — the same tissue where peritoneal endometriosis implants can form. Understanding the anatomy of the peritoneal cavity helps explain how endometrial cells can attach, spread, and cause inflammation throughout the abdomen.
COMMON QUESTIONS ABOUT Peritoneal Endometriosis
What are the Subtypes of Peritoneal Endometriosis?
There are different subtypes of peritoneal endometriosis based on the location and characteristics of the endometrial implants within the peritoneum. Some of the common subtypes include:
- Superficial peritoneal endometriosis: This subtype involves small, superficial implants or lesions on the surface of the peritoneum.
- Deep infiltrating peritoneal endometriosis (DIPE): In this subtype, endometrial tissue infiltrates deeply into the peritoneal tissue, extending beyond the surface. It can involve structures such as the bowel, bladder, ureters, and pelvic sidewalls.
- Ovarian endometriosis: This subtype specifically refers to the presence of endometriosis on or within the ovaries, forming cysts called endometriomas.
- Rectovaginal endometriosis: This subtype involves the presence of endometrial implants between the rectum and the vagina, causing pain, inflammation, and potential complications.
These subtypes can coexist or occur individually, and the severity and symptoms can vary from person to person. Proper diagnosis and classification of the subtype are important for effective management and treatment planning
Why is Peritoneal Endometriosis So Unique?
Peritoneal endometriosis is a unique condition because it involves the abnormal growth of endometrial tissue outside the uterus, specifically on the peritoneum, which is the tissue lining the abdominal cavity. Here are a few reasons why peritoneal endometriosis is considered unique:
Location: Peritoneal endometriosis occurs in the peritoneal cavity, which is an uncommon site for endometrial tissue growth. Normally, endometrial tissue is found lining the inner wall of the uterus. When it grows outside the uterus, it can implant on various structures within the peritoneal cavity, such as the ovaries, fallopian tubes, bladder, intestines, and other abdominal organs.
Mechanism of spread: The exact cause of endometriosis is not fully understood, but there are several theories. One theory is retrograde menstruation, where menstrual blood containing endometrial cells flows backward through the fallopian tubes into the pelvic cavity. However, the spread of endometriosis to the peritoneal cavity involves additional factors that allow the endometrial cells to attach, invade, and grow on the peritoneal surface.
Diverse symptoms: Peritoneal endometriosis can present with a wide range of symptoms, including pelvic pain, painful periods, pain during intercourse, irregular bleeding, infertility, and gastrointestinal symptoms such as bloating, constipation, or diarrhea. The symptoms can vary in intensity and may not always correlate with the severity of the condition.
Diagnostic challenges: Diagnosing peritoneal endometriosis can be challenging because its symptoms overlap with other conditions such as pelvic inflammatory disease, irritable bowel syndrome, and ovarian cysts. Additionally, the gold standard for definitive diagnosis is through laparoscopic surgery with tissue biopsy, which is an invasive procedure.
Impact on fertility: Peritoneal endometriosis can affect fertility by causing inflammation, scarring, and adhesions that can impair the function of the ovaries, fallopian tubes, and uterus. The abnormal tissue growth and associated structural changes can disrupt the normal processes of ovulation, fertilization, and implantation, making it more difficult for a woman to conceive.
Recurrence and persistence: Peritoneal endometriosis can be a chronic condition with a tendency to recur even after surgical removal or medical treatment. This is because some endometrial cells may remain or regrow after treatment, and the hormonal fluctuations during the menstrual cycle can stimulate their growth.
It’s important to note that while peritoneal endometriosis is unique in its characteristics, there are other forms of endometriosis, such as ovarian endometriosis and deep infiltrating endometriosis, which also have their own distinctive features.
How is Peritoneal Endometriosis Diagnosed?
The diagnosis of peritoneal endometriosis typically involves a combination of medical history evaluation, physical examination, imaging tests, and, in many cases, a definitive confirmation through surgical intervention. Here are the common steps involved in diagnosing peritoneal endometriosis:
Medical history and symptom evaluation: The doctor will review your medical history and ask about your symptoms, such as pelvic pain, painful periods, infertility, or gastrointestinal issues. Providing detailed information about the nature, severity, and timing of your symptoms can assist in the diagnostic process.
Physical examination: A pelvic examination may be performed to check for any abnormalities, tenderness, or masses in the pelvic region. However, it’s important to note that physical examination alone cannot provide a definitive diagnosis of peritoneal endometriosis.
Imaging tests: Imaging studies such as transvaginal ultrasound (TVUS) or pelvic ultrasound may be conducted to visualize the pelvic organs and look for any signs of endometriosis, such as ovarian cysts (endometriomas) or deep infiltrating lesions. However, these imaging tests may not always provide conclusive evidence of peritoneal endometriosis.
Laparoscopy: Laparoscopic surgery is considered the gold standard for the diagnosis of peritoneal endometriosis. It is a minimally invasive procedure where a thin, lighted tube with a camera (laparoscope) is inserted through small incisions in the abdomen. This allows the surgeon to directly visualize and examine the pelvic organs and peritoneum for the presence of endometrial implants, adhesions, and other characteristic signs of endometriosis. Tissue samples (biopsies) may also be taken during laparoscopy for histological examination to confirm the presence of endometrial tissue.
It’s important to consult with a healthcare professional who specializes in endometriosis diagnosis and treatment for an accurate evaluation and management of peritoneal endometriosis. Each case is unique, and the diagnostic process may vary depending on individual circumstances.
How does the immune system affect peritoneal endometriosis?
Peritoneal endometriosis involves the presence of endometrial tissue outside the uterus, specifically within the peritoneal cavity. The immune system plays a crucial role in the development and progression of endometriosis, including peritoneal endometriosis. Here’s how the immune system interacts with peritoneal endometriosis:
Inflammatory response: The presence of endometrial tissue outside the uterus triggers an inflammatory response within the peritoneal cavity. Immune cells, such as macrophages and T cells, are recruited to the affected areas and release various inflammatory molecules and cytokines. This inflammation contributes to the symptoms associated with peritoneal endometriosis, such as pelvic pain and tissue damage.
Immune cell dysfunction: In women with peritoneal endometriosis, there is evidence of altered immune cell function. Some studies have shown that immune cells in the peritoneal fluid of affected individuals exhibit impaired ability to recognize and eliminate endometrial cells, leading to their survival and growth outside the uterus.
Immune tolerance: Endometriosis is characterized by the ability of endometrial cells to evade immune surveillance and establish themselves in ectopic locations. The immune system may exhibit a certain degree of tolerance towards these misplaced endometrial cells, failing to mount a robust immune response to eliminate them. This immune tolerance allows the survival and growth of endometrial implants within the peritoneal cavity.
Inflammatory mediators: The immune cells and endometrial tissue in the peritoneal cavity produce various inflammatory mediators, such as prostaglandins, cytokines, and growth factors. These molecules contribute to the development and progression of peritoneal endometriosis by promoting tissue invasion, angiogenesis (formation of new blood vessels), and the formation of adhesions between organs.
Hormonal influence: Hormones, particularly estrogen, have a significant impact on the immune response and the growth of endometriotic tissue. Estrogen can modulate immune cell function and promote the survival and proliferation of endometrial cells. It is believed that hormonal imbalances and increased estrogen levels contribute to the development and maintenance of peritoneal endometriosis.
Understanding the complex interplay between peritoneal endometriosis and the immune system is crucial for developing targeted treatment strategies. Research in this area aims to identify immune-based therapies that can modulate the immune response and improve outcomes for individuals with peritoneal endometriosis.
Surgical Treatment for Peritoneal endometriosis
Surgical treatment is often an important approach for managing peritoneal endometriosis, particularly when the symptoms are severe or when fertility preservation is a concern. The primary goal of surgical treatment is to remove or ablate the endometrial implants, alleviate symptoms, and restore normal anatomical structures within the peritoneal cavity. Here are some common surgical options for peritoneal endometriosis:
Laparoscopic Excision
Laparoscopic surgery, also known as minimally invasive or keyhole surgery, is the preferred approach for treating peritoneal endometriosis. During the procedure, small incisions are made in the abdomen, and a laparoscope (a thin, lighted tube with a camera) is inserted to visualize the pelvic organs and the peritoneal cavity. Surgical instruments are used to excise or remove the endometrial implants, adhesions, and any other abnormal tissue. This technique allows for a precise and targeted removal of the endometriotic lesions while minimizing trauma to surrounding tissues.
On average, the cost of laparoscopic excision for endometriosis can range from approximately $7,000 to $15,000 or more.
To obtain an accurate cost estimate, it is advisable to arrange an appointment with New York Gynecology Surgery & Endometriosis (NYGSE).
Laser Ablation
Laser ablation is a technique that uses laser energy to destroy or vaporize the endometrial implants. It is performed during laparoscopic surgery and can be effective for superficial lesions or areas that are difficult to excise. The laser energy is applied to the lesions, effectively destroying the abnormal tissue.
Deep Infiltrating Endometriosis (DIE) Surgery
In cases where peritoneal endometriosis involves deep infiltration into surrounding tissues or organs, a more extensive surgical procedure may be required. This type of surgery aims to remove the deeply infiltrating endometrial implants and restore the affected organs’ normal anatomy and function. It may involve excision, resection, or reconstruction of the affected organs, such as the bowel, bladder, or ureters. DIE surgery is often performed by experienced specialists in endometriosis and may require collaboration with other surgical specialties.
Service Areas
NYGSE provides care for patients throughout Babylon and Bay Shore, NY experiencing peritoneal endometriosis, emphasizing accurate diagnosis and targeted treatment for disease located along the surface of the pelvic cavity.
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Have Questions About Your Surgery or Treatment?
Expert treatment. Compassionate care. Real results.
November 17, 2025by admin
What is Endometriosis?
What Is Endometriosis?
Endometriosis is a chronic condition in which tissue similar to the uterine lining grows outside the uterus, causing inflammation, scarring, and often significant pain. These lesions can develop on the ovaries, fallopian tubes, bowel, bladder, and other pelvic structures, sometimes affecting organs beyond the pelvis. Endometriosis can lead to painful periods, pelvic pain, painful intercourse, heavy bleeding, digestive symptoms, and fertility challenges. Because symptoms vary widely and often overlap with other conditions, many individuals experience delays in diagnosis, making early evaluation by an experienced specialist essential.
This illustration shows the female reproductive organs with endometrial-like tissue growing outside the uterus. These lesions can appear on the ovaries, fallopian tubes, and pelvic peritoneum, contributing to inflammation, scar tissue, and pain. Understanding where endometriosis forms helps explain the wide range of symptoms and why accurate diagnosis often requires specialized evaluation.
COMMON QUESTIONS ABOUT Endometriosis
Where Does Endometriosis Occur?
Endometriosis occurs when tissue similar to the lining of the uterus grows outside of the uterus, often in other areas of the pelvis such as the ovaries, fallopian tubes, bowel, bladder, or the lining of the pelvis itself.
It is frequently found on the top of the vagina (anterior cul-de-sac) and in the peritoneal cavity between the rectum and the posterior wall of the uterus (posterior cul-de-sac).
In some exceptional instances, it may spread to other areas of the body, including the diaphragm, lungs, kidney, appendix, and even the gastrocnemius muscles in the calf.
What causes endometriosis?
The exact cause of endometriosis is not yet fully understood, but there are several theories.
One theory suggests that it may occur due to retrograde menstruation, where menstrual blood and endometrial tissue flow back through the fallopian tubes and into the pelvis during menstruation.
Another theory suggests that it may be caused by genetics or a problem with the immune system that allows the endometrial tissue to grow outside the uterus. Hormonal factors, such as excess estrogen production, may also contribute to the development of endometriosis.
However, the precise cause or causes of endometriosis remain a subject of ongoing research.
What are the symptoms of endometriosis?
Endometriosis can manifest in various symptoms, with pain being the primary indicator. This pain may vary from mild to severe and typically affects the abdomen, pelvic region, and lower back.
While some individuals with endometriosis may not experience symptoms, others may encounter:
- painful menstrual cramps
- abdominal or back pain during and in between periods
- pain during intercourse
- heavy bleeding
- spotting between periods
- infertility
- painful bowel movements.
The severity of the symptoms does not necessarily correspond with the extent of the endometriosis; a person with limited patches may experience severe pain while someone with severe endometriosis may not have much discomfort.
What are the Stages of Endometriosis?
Endometriosis can be classified into four stages or types, based on the location, size, and depth of the endometrial tissue growth:
- Minimal or Stage 1: In this stage, there are small lesions or shallow implants on the surface of the ovary and pelvic lining.
- Mild or Stage 2: In this stage, there are more lesions and deeper implants in the pelvic lining and on the ovary.
- Moderate or Stage 3: This stage involves deep implants on the pelvic lining and ovaries, as well as the formation of adhesions (scar tissue) between organs.
- Severe or Stage 4: This is the most advanced stage of endometriosis, in which deep implants and adhesions are widespread throughout the pelvic cavity, affecting multiple organs such as the bladder, rectum, and intestines.
It is important to note that the stage of endometriosis does not necessarily correlate with the severity of symptoms, as individuals with minimal endometriosis may experience significant pain while those with severe endometriosis may be asymptomatic.
How is endometriosis diagnosed?
What is the Initial Step in Diagnosing Endometriosis?
To determine whether imaging tests are necessary, it is recommended to first consult with a GYN physician who is experienced in diagnosing endometriosis and can perform a thorough pelvic exam, including a discussion of your symptoms and medical history.
What Imaging Test are Available?
There are several imaging tests that can be used to help diagnose endometriosis. These include transvaginal ultrasound, magnetic resonance imaging (MRI), and computed tomography (CT) scan.
- Transvaginal Ultrasound is a type of imaging test that may be used to diagnose or evaluate endometriosis. It involves inserting an ultrasound wand into the vagina to create images of the reproductive organs and surrounding structures. This can help to identify the presence of endometriotic cysts or lesions in the ovaries or other areas. However, it is important to note that not all cases of endometriosis can be detected through ultrasound, and other imaging tests or diagnostic procedures may be necessary.
- Magnetic resonance imaging (MRI) can also be used to diagnose endometriosis. This imaging technique uses a powerful magnet and radio waves to create detailed images of the inside of the body. It can provide information on the location and extent of endometriosis lesions, as well as identify any potential complications such as cysts or adhesions. An MRI can also be useful in ruling out other conditions that may be causing similar symptoms. However, MRI is not typically used as a first-line diagnostic tool for endometriosis and may be more expensive and time-consuming than other imaging tests.
Gold Standard for Diagnosing Endometriosis
Laparoscopy is a surgical procedure that is commonly used to diagnose and treat endometriosis. During a laparoscopy, a surgeon makes a small incision near the navel and inserts a thin, lighted instrument called a laparoscope into the abdomen. The laparoscope allows the surgeon to view the pelvic organs and look for signs of endometrial tissue outside the uterus. If endometriosis is found, the surgeon may also remove the tissue during the same procedure.
Laparoscopy is considered the gold standard for diagnosing endometriosis.
How do hormonal treatments work for endometriosis management?
Hormonal treatments for endometriosis management work by changing the hormone signals that can stimulate endometriosis tissue and worsen inflammation, pelvic pain, and painful periods. Since endometriosis symptoms often flare with the menstrual cycle, these medications may help by suppressing ovulation, reducing or stopping menstrual bleeding, lowering estrogen activity, or thinning the uterine lining.
Common hormonal options may include progestin-only birth control pills, hormonal IUDs, GnRH agonists, GnRH antagonists, and other medications that temporarily reduce hormone-driven disease activity. These treatments may help some patients manage symptoms, but they do not remove endometriosis lesions or provide a complete cure.
At NYGSE, hormonal therapy may be considered part of symptom management, but patients with persistent pain, advanced endometriosis, deep infiltrating disease, bowel or bladder involvement, ovarian endometriomas, or fertility concerns may need a more comprehensive evaluation. For many patients, laparoscopic deep excision surgery combined with a multidisciplinary treatment plan offers the most complete approach to treating endometriosis.
Surgical Methods for Endometriosis Treatment
There are several surgical methods for treating endometriosis, including laparoscopic excision, robotic-assisted laparoscopy, and laparotomy. The specific method used depends on the severity and location of the endometrial tissue, as well as the patient’s overall health and preferences. In general, the goal of surgery for endometriosis is to remove the affected tissue while preserving healthy tissue and organs as much as possible.
What is laparoscopic excision for endometriosis?
Laparoscopic excision is a surgical procedure that can be used to remove endometriosis tissue from the body. It involves making small incisions in the abdomen and inserting a laparoscope (a thin, lighted tube with a camera) to visualize the internal organs. Surgical instruments are then used to remove the endometrial tissue. This procedure is considered the gold standard for diagnosing and treating endometriosis.
The cost of laparoscopic excision of endometriosis can vary depending on the location, healthcare provider, and type of insurance. It’s recommended to request an appointment with New York Gynecology Surgery & Endometriosis (NYGSE) to obtain an accurate estimate of the cost.
What is robotic-assisted laparoscopy for endometriosis?
Robotic-assisted laparoscopy is a type of laparoscopic surgery that uses a computer-controlled robot to perform the surgery. It is a minimally invasive surgical option that can be used to diagnose and treat endometriosis. The cost of robotic-assisted laparoscopy for endometriosis will vary depending on factors such as the hospital or surgical center, surgeon fees, and insurance coverage.
However, in general, robotic-assisted laparoscopy is often more expensive than traditional laparoscopy due to the use of the robot and the associated technology.
What is Laparotomy?
Laparotomy is a surgical procedure that involves making a large incision in the abdominal wall to gain access to the pelvic organs. It is used to diagnose and treat a variety of conditions, including endometriosis. During laparotomy for endometriosis, the surgeon will make an incision in the abdominal wall, and then carefully remove the endometrial tissue. Laparotomy is a more invasive surgery than laparoscopy and is typically reserved for cases where the endometrial tissue is widespread or in hard-to-reach areas.
However, it may also be recommended in cases where a woman has a large mass or adhesions that need to be removed. The recovery time for laparotomy is longer than that for laparoscopy.
The cost of laparotomy can vary depending on the location, healthcare provider, and individual circumstances.
Non-surgical methods for endometriosis treatment
Although non-surgical treatments like NSAIDs, progestin-only birth control pills, and GnRH analogs can alleviate some symptoms of endometriosis, they are usually temporary and do not provide a complete cure for the disease. The most effective approach to treating endometriosis involves undergoing laparoscopic deep excision surgery and a comprehensive multidisciplinary treatment plan.
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Have Questions About Your Surgery or Treatment?
Expert treatment. Compassionate care. Real results.
November 17, 2025by admin
Ovarian Endometrioma
Understanding Ovarian Endometriomas (Chocolate Cyst)
An ovarian endometrioma—often called a “chocolate cyst”—is a type of ovarian cyst formed when endometrial-like tissue grows inside the ovary and collects old, dark blood. These cysts are strongly associated with endometriosis and can lead to pelvic pain, menstrual irregularities, painful intercourse, bloating, and fertility challenges. While some endometriomas remain small and asymptomatic, others can grow, rupture, or cause significant inflammation. Accurate diagnosis and individualized treatment are important for managing symptoms and protecting ovarian function.
This illustration shows the female reproductive anatomy with an endometrioma forming inside the ovary. Endometrial-like tissue can implant on the ovary and accumulate dark, old blood, creating what is commonly referred to as a “chocolate cyst.” Visualizing where endometriomas develop helps explain symptoms such as pelvic pain, bloating, and infertility, and highlights the connection between ovarian cysts and endometriosis.
COMMON QUESTIONS ABOUT Ovarian Endometrioma
How Do Chocolate Cysts in the Ovaries Form?
Retrograde menstruation is believed to be one of the possible causes of endometriosis, but it is not the only cause. Retrograde menstruation occurs when menstrual blood containing endometrial cells flows back through the fallopian tubes and into the pelvic cavity instead of leaving the body through the vagina. As a result, blood accumulates in the ovaries, leading to the development of an endometrioma (chocolate cysts).
In women with endometriosis, it is thought that these endometrial cells can implant and grow on other organs in the pelvic cavity, leading to the development of endometriosis. However, not all women who experience retrograde menstruation develop endometriosis, and other factors such as hormonal imbalances and immune dysfunction may also play a role.
Other theories for the cause of endometriosis include genetic predisposition, environmental factors, and abnormalities in the development of the reproductive system. The exact cause of endometriosis is still not fully understood and more research is needed to better understand the condition.
Why are Ovarian Endometriomas Called “Chocolate Cysts?
Ovarian endometriomas are referred to as “chocolate cysts” because of the dark, reddish-brown fluid that fills them, resembling chocolate. These cysts have the potential to rupture suddenly, causing their contents to spill and adhere to the abdominal cavity’s nearby organ walls.
What are the Symptoms of Ovarian Endometrioma?
The symptoms of ovarian endometrioma or chocolate cysts can vary from person to person. Some common symptoms include:
- Pelvic pain: Dull or sharp pain in the lower abdomen or pelvis that may become more severe during menstruation.
- Menstrual irregularities: Heavy or irregular menstrual bleeding, or spotting between periods.
- Pain during sex: Pain or discomfort during sexual intercourse.
- Infertility: Difficulty getting pregnant or experiencing recurrent miscarriages.
- Digestive symptoms: Bloating, constipation, or diarrhea.
In some cases, ovarian endometriomas may not cause any noticeable symptoms, and they are discovered incidentally during a routine pelvic exam or imaging test. It is important to talk to a doctor if you experience any persistent symptoms or have concerns about your reproductive health.
How is Ovarian Endometrioma Diagnosed?
The diagnosis of ovarian endometrioma or chocolate cysts typically involves a combination of medical history, physical examination, and imaging tests.
During the physical examination, a doctor may perform a pelvic exam to check for any abnormalities or pain. They may also order imaging tests such as an ultrasound, MRI, or CT scan to confirm the presence of an ovarian cyst and determine its size, shape, and location.
In some cases, a doctor may recommend a laparoscopy, which is a surgical procedure that involves making small incisions in the abdomen to insert a camera and other instruments to visualize and biopsy the cyst.
Additionally, blood tests may be conducted to check for markers of endometriosis or other underlying conditions. A definitive diagnosis of ovarian endometrioma is usually confirmed by microscopic examination of the tissue obtained through biopsy or surgical removal.
Surgical Methods for Ovarian Endometrioma Treatment
There are several surgical methods for treating ovarian endometrioma, including laparoscopic cystectomy, robotic-assisted laparoscopy, and laparotomy. The specific method used depends on the severity and location of the endometrial tissue, as well as the patient’s overall health and preferences. In general, the goal of surgery for ovarian endometrioma is to remove the affected tissue while preserving healthy tissue and organs as much as possible.
Laparoscopic Cystectomy
Laparoscopic cystectomy is a surgical procedure that involves the removal of an ovarian cyst, such as an ovarian endometrioma or chocolate cyst, using minimally invasive techniques.
During the procedure, the surgeon makes small incisions in the abdomen and inserts a laparoscope, which is a thin, lighted tube with a camera attached to it, and other surgical instruments. The camera provides real-time images of the cyst and surrounding tissue, allowing the surgeon to carefully remove the cyst while minimizing damage to healthy tissue.
Laparoscopic cystectomy is generally considered a safe and effective treatment option for ovarian endometriomas, and it has several advantages over traditional open surgery, including smaller incisions, less pain and scarring, and a shorter recovery time. However, as with any surgery, there are some risks and potential complications, including bleeding, infection, damage to surrounding organs, and recurrence of the cyst.
Robotic-Assisted Laparoscopy
Ovarian endometrioma robotic-assisted laparoscopy is a minimally invasive surgical procedure used to remove endometrial tissue that has grown inside the ovary while preserving the ovarian function.
Robotic-assisted laparoscopy is a type of laparoscopic surgery that uses robotic arms to perform the surgery instead of a surgeon’s hands. This technology allows for greater precision and control during the procedure, and can result in less pain, scarring, and a faster recovery time compared to traditional open surgery.
The cost of ovarian endometrioma robotic-assisted laparoscopy can vary depending on several factors, including your location, the complexity of the surgery, and your insurance coverage.
Ovarian Endometrioma Laparotomy
Ovarian endometrioma laparotomy is a surgical procedure used to remove endometrial tissue that has grown inside the ovary. Laparotomy is an open surgery that involves making a larger incision in the abdomen to access the affected ovary.
The cost of ovarian endometrioma laparotomy can vary depending on several factors, including your location, the complexity of the surgery, and your insurance coverage.
Service Areas
NYGSE cares for patients throughout Babylon and Bay Shore, NY with ovarian endometriomas, using advanced imaging and surgical techniques to manage cysts effectively while supporting long-term reproductive and pelvic health.
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.