
November 17, 2025by admin
Rectal Endometriosis
Understanding Rectal Endometriosis
Rectal endometriosis occurs when endometrial-like tissue grows on, around, or within the rectal wall. Because the rectum is part of the lower digestive tract, this form of endometriosis can cause significant pain, bleeding, and bowel dysfunction—especially during menstruation. Although less common than pelvic or ovarian endometriosis, rectal involvement is often associated with deeper, more advanced disease. Early evaluation and an accurate diagnosis are essential for choosing the right treatment approach, which may include medication, minimally invasive surgery, or coordinated care with colorectal specialists.
This illustration shows the lower digestive tract, highlighting where rectal endometriosis can develop. Endometrial-like tissue may implant on the rectal surface or invade deeper layers of the rectal wall, causing inflammation, bleeding, and pain during bowel movements. Visualizing the rectum in relation to the surrounding intestines helps explain why symptoms often overlap with other gastrointestinal disorders.
COMMON QUESTIONS ABOUT Rectal Endometriosis
What are the Causes of Rectal Endometriosis?
The exact causes of rectal endometriosis are not fully understood, but there are several theories and factors that may contribute to its development. Here are some possible causes and contributing factors:
- Retrograde menstruation: Retrograde menstruation is a common theory for the development of endometriosis in general, including rectal endometriosis. It occurs when menstrual blood containing endometrial cells flows backward through the fallopian tubes and into the pelvic cavity instead of being expelled through the vagina. These endometrial cells can then implant and grow on various organs, including the rectum.
- Metaplasia: Metaplasia refers to the transformation of normal cells into endometrial-like cells. It is believed that certain cells in the pelvic region can undergo metaplasia and develop into endometrial tissue outside the uterus, including in the rectal area.
- Immune system dysfunction: It is thought that immune system dysfunction or alterations may contribute to the development of endometriosis. In a healthy immune system, immune cells would recognize and eliminate endometrial cells that have implanted outside the uterus. However, in individuals with endometriosis, the immune response may be impaired, allowing the endometrial cells to persist and grow.
- Genetic factors: There may be a genetic predisposition to endometriosis, including rectal endometriosis. If a close family member, such as a mother or sister, has endometriosis, the risk of developing the condition may be higher.
- Hormonal imbalances: Hormonal factors play a significant role in the growth and shedding of the endometrial tissue. It is believed that hormonal imbalances, particularly involving estrogen, may contribute to the development and progression of endometriosis. Estrogen can promote the growth of endometrial tissue outside the uterus, including in the rectal area.
It’s important to note that while these factors are associated with the development of endometriosis, they may not be the sole causes. The exact interplay of these factors and the individual’s susceptibility to endometriosis is still being researched.
What are the Different Types of Rectal Endometriosis?
Rectal endometriosis can be classified into different types based on the depth of infiltration and the extent of involvement. The classification helps in understanding the severity of the condition and determining appropriate treatment strategies. Here are the commonly recognized types of rectal endometriosis:
- Superficial endometriosis: Superficial rectal endometriosis refers to the presence of endometrial implants on the surface of the rectum or the peritoneum covering the rectum. In this type, the endometrial tissue does not penetrate deeply into the rectal wall.
- Nodular endometriosis: Nodular rectal endometriosis involves the formation of nodules or masses within the rectal wall. These nodules can be palpable during a rectal examination and may cause symptoms such as pain, bleeding, or bowel dysfunction.
- Deep infiltrating endometriosis (DIE): Deep infiltrating endometriosis is the most severe and extensive form of rectal endometriosis. In this type, the endometrial tissue penetrates deeply into the rectal wall and can extend beyond the rectum, involving nearby structures such as the vagina, bladder, or pelvic sidewalls. DIE can cause significant pain, bowel dysfunction, and other symptoms.
- Rectovaginal endometriosis: Rectovaginal endometriosis is a subtype of rectal endometriosis that specifically involves the area between the rectum and the vagina. It can result in the formation of nodules or adhesions that affect both the rectal and vaginal walls. This type often causes pain during intercourse and other symptoms related to both the rectum and vagina.
It’s important to note that these classifications are not mutually exclusive, and an individual may have a combination of different types of rectal endometriosis. The classification helps in determining the severity of the disease and guiding treatment decisions, including surgical approaches and the involvement of multidisciplinary teams.
Proper diagnosis and classification of rectal endometriosis are typically made through a combination of medical history review, physical examination, imaging studies (such as ultrasound or MRI), and sometimes a diagnostic laparoscopy.
How is Rectal Endometriosis Diagnosed?
The diagnosis of rectal endometriosis typically involves a comprehensive evaluation by a healthcare professional, often an endometriosis specialist or a team of specialists, to accurately assess the condition. Here are the main steps and methods involved in diagnosing rectal endometriosis:
- Medical history review: The healthcare professional will begin by discussing your symptoms, medical history, and any previous diagnoses or treatments related to endometriosis. They will ask specific questions about your bowel habits, rectal pain, bleeding, and other related symptoms.
- Physical examination: A pelvic examination may be performed to assess any abnormalities, tenderness, or masses in the pelvic region. A digital rectal examination may also be conducted to evaluate the rectum and detect any palpable nodules or abnormalities.
- Imaging studies: Imaging techniques can provide visual information about the pelvic organs and help identify any endometrial implants or structural abnormalities. The following imaging studies may be used:
- Ultrasound: Transvaginal or transrectal ultrasound can provide detailed images of the pelvic organs, including the rectum, and help identify endometrial implants or nodules.
- Magnetic Resonance Imaging (MRI): MRI can provide more detailed imaging of the pelvis and help visualize the extent of endometriosis, including the involvement of the rectum and surrounding structures.
- Colonoscopy or sigmoidoscopy: These procedures involve the insertion of a thin, flexible tube with a camera into the rectum and colon to directly visualize the lining and identify any endometrial implants or lesions. Biopsies may also be taken during these procedures to confirm the presence of endometrial tissue.
- Diagnostic laparoscopy: Laparoscopy is a surgical procedure performed under general anesthesia to directly visualize the pelvic organs and confirm the presence of endometriosis. During laparoscopy, a small incision is made near the navel, and a thin, lighted instrument called a laparoscope is inserted to examine the pelvic region. If rectal endometriosis is suspected, the surgeon may specifically focus on assessing the rectal area and obtain tissue samples (biopsies) for further analysis.
It’s important to note that a definitive diagnosis of rectal endometriosis often requires visualization and confirmation through laparoscopy, as other imaging techniques may not always provide a conclusive diagnosis. A multidisciplinary approach involving gynecologists, colorectal surgeons, and radiologists may be necessary for accurate diagnosis and treatment planning.
What is the Difference Between Rectal and Bowel Endometriosis?
Rectum and bowel endometriosis are both types of endometriosis that involve the gastrointestinal tract, but they refer to different areas within the digestive system.
Rectum endometriosis specifically refers to the presence of endometrial tissue within or around the rectum. The rectum is the final portion of the large intestine, located just above the anus. When endometrial tissue implants on or near the rectal wall, it can cause symptoms such as rectal pain, bleeding during bowel movements, and painful bowel movements.
On the other hand, bowel endometriosis refers to the involvement of the bowel as a whole, which includes the rectum as well as other parts of the intestine. Bowel endometriosis can affect different sections of the bowel, including the small intestine, large intestine (colon), and rectum. The extent of involvement can vary from superficial implants on the bowel surface to deep infiltration into the bowel wall.
The symptoms of bowel endometriosis can be similar to those of rectum endometriosis and may include rectal pain, bleeding during bowel movements, painful bowel movements, constipation, diarrhea, and abdominal pain. In some cases, bowel endometriosis can lead to bowel obstruction or strictures, which can cause severe abdominal pain and affect normal bowel movements.
Surgical Methods for Rectal Endometriosis Treatment
Surgical intervention is often required to effectively treat rectal endometriosis. Here are some surgical methods commonly used for rectal endometriosis treatment:
Rectal Laparoscopic Excision
Rectal laparoscopic excision, also known as rectal shaving or rectal nodule resection, is a surgical procedure performed to remove endometriotic lesions affecting the rectum. It is a minimally invasive approach that offers several advantages over open surgery, including smaller incisions, reduced scarring, shorter recovery time, and less post-operative pain.
It’s worth noting that rectal laparoscopic excision is typically performed by gynecological surgeons or colorectal surgeons who have expertise in treating endometriosis. The specific details of the surgery may vary depending on the extent and location of the rectal endometriosis, as well as the surgeon’s preferences and techniques.
Robotic-Assisted Laparoscopy
Rectal robotic-assisted laparoscopy, also known as robotic-assisted rectal surgery, is a surgical technique that combines laparoscopic surgery with robotic technology to perform rectal procedures. It involves using the da Vinci Surgical System or a similar robotic platform to enhance the surgeon’s precision, control, and visualization during the procedure.
The use of robotic technology in rectal surgery offers several potential advantages, including improved visualization, enhanced precision, and reduced risk of complications. However, it’s important to note that not all rectal surgeries require robotic assistance, and the decision to use robotic-assisted laparoscopy is based on the surgeon’s judgment and the patient’s specific condition.
Bowel Resection
Bowel resection is a surgical procedure that may be performed to treat rectal endometriosis when the disease has deeply infiltrated the rectal wall or involves a significant portion of the bowel. It involves removing the affected segment of the rectum and rejoining the healthy ends of the bowel. Bowel resection aims to eliminate the endometriotic lesions and restore normal bowel function.
It’s important to note that bowel resection is a major surgical procedure and carries potential risks and complications, including bleeding, infection, anastomotic leakage, bowel obstruction, and the need for a permanent colostomy in rare cases. The decision to perform bowel resection for rectal endometriosis is typically made based on factors such as the severity of the disease, symptoms, and the patient’s desire for fertility preservation.
Service Areas
Patients in Babylon and Bay Shore, NY diagnosed with rectal endometriosis can rely on NYGSE for advanced care, where complex bowel involvement is carefully evaluated and treated with precise surgical techniques.

Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Expert treatment. Compassionate care. Real results.
November 17, 2025by admin
Bowel Endometriosis
Understanding Bowel Endometriosis
Bowel endometriosis occurs when endometrial-like tissue grows on or within the small or large intestine. Because the bowel plays a major role in digestion and movement of stool, these lesions can cause significant discomfort, including abdominal pain, bloating, constipation, diarrhea, and painful bowel movements. Symptoms often overlap with other gastrointestinal conditions, which can make diagnosis challenging. Understanding how endometriosis affects the bowel helps guide proper evaluation and individualized treatment. Why did you go to gymnastics
This illustration highlights the small and large intestines, where bowel endometriosis can develop. When endometrial-like tissue implants on or penetrates the bowel wall, it can trigger inflammation, pain, and disruptive digestive symptoms. Understanding how endometriosis affects the bowel helps clarify why some patients experience gastrointestinal issues that overlap with other GI conditions.
COMMON QUESTIONS ABOUT Bowel Endometriosis
What are the Two Forms of Bowel Endometriosis?
There are two forms of bowel endometriosis:
- Superficial bowel endometriosis: In this form, endometrial tissue grows on the surface of the bowel, and may cause symptoms such as abdominal pain, bloating, and changes in bowel movements.
- Deep infiltrating bowel endometriosis: This is a more severe form, where endometrial tissue grows deeply into the bowel wall, and may cause symptoms such as severe abdominal pain, constipation, diarrhea, and rectal bleeding. In some cases, deep infiltrating bowel endometriosis can lead to bowel obstruction or perforation, which requires emergency medical attention.
What are the Causes of Bowel Endometriosis?
The exact causes of this condition are not fully understood, several theories have been proposed. One theory is that during menstruation, the blood containing endometrial cells flows back through the fallopian tubes into the pelvic cavity, where the cells implant and grow on the bowel. Another theory suggests that endometrial cells may spread through the bloodstream or lymphatic system to reach the bowel. Hormones, such as estrogen, may also play a role in the development of bowel endometriosis, as they can stimulate the growth of endometrial tissue.
In addition to these factors, genetic predisposition may also contribute to the development of bowel endometriosis. Studies have suggested that certain genetic variations may increase the risk of developing endometriosis. Other risk factors for endometriosis include early onset of menstruation, heavy or prolonged menstrual periods, and a family history of the condition. However, it’s important to note that not all women with these risk factors will develop bowel endometriosis, and some women without any known risk factors may still develop the condition. More research is needed to fully understand the causes of bowel endometriosis.
What are the Symptoms of Bowel Endometriosis?
Bowel endometriosis can cause a range of symptoms, which may vary in severity depending on the extent of the endometrial tissue growth. Some common symptoms of bowel endometriosis include:
- Abdominal pain or cramping: This can be mild to severe and may be felt in the lower abdomen or pelvic region.
- Bloating: Bowel endometriosis can cause the bowel to become distended, leading to bloating and discomfort.
- Changes in bowel movements: These can include constipation, diarrhea, or both, and may be accompanied by abdominal pain or cramping.
- Rectal bleeding: In some cases, bowel endometriosis can cause bleeding from the rectum, especially during or after bowel movements.
- Pain during bowel movements: This can be a sharp, stabbing pain or a more dull ache, and may be accompanied by cramping.
- Pain during sexual intercourse: Bowel endometriosis can cause pain or discomfort during sex, particularly during deep penetration.
It’s important to note that these symptoms can be caused by other conditions as well, and not all women with bowel endometriosis will experience all of these symptoms. If you are experiencing any of these symptoms, it’s important to request an appointment with New York Gynecology Surgery & Endometriosis (NYGSE) to determine the underlying cause and appropriate endometriosis treatment.
How is Bowel Endometriosis Diagnosed?
Around 10%-12% of women of reproductive age are affected by endometriosis, which is usually diagnosed in women in their 30s. If you’re experiencing symptoms of endometriosis, your doctor will begin by inquiring about your medical history and symptoms, and then conduct a pelvic exam. Depending on the findings, imaging tests may be recommended to provide more information about any cysts or tissue damage associated with endometriosis. These imaging tests may include:
- A transvaginal or transrectal ultrasound involves inserting a wand-like device into your vagina or rectum, which emits sound waves to create images of your organs. While this test cannot diagnose endometriosis, it can locate lesions that may be caused by endometriosis once they have grown large enough to be detected.
- MRI or magnetic resonance imaging is a diagnostic test that produces detailed images of your organs and tissues by using a combination of a magnetic field and radio waves.
- Laparoscopy is a procedure in which a surgeon creates a small incision near your belly button and inserts a laparoscope, a thin viewing tool, to examine your internal organs. This procedure is sometimes used to remove lesions caused by endometriosis.
- Barium enema is a type of X-ray that helps doctors to identify changes or abnormalities in your large intestine (colon). To perform this test, a liquid and barium mixture is injected into your rectum through a small tube. This mixture expands your intestine and air is pumped in to improve image quality.
Surgical Methods for the Treatment of Bowel Endometriosis
The surgical methods for treating bowel endometriosis depend on the specific type and severity of the anomaly, as well as the individual patient’s circumstances and reproductive goals. The surgical treatment for bowel endometriosis may involve laparoscopic excision surgery, bowel resection surgery or robotic-assisted surgery.
Laparoscopic Excision Surgery
Laparoscopic excision surgery involves the removal of the endometrial tissue using a laparoscope, a thin viewing tool with a light and camera attached to it. This minimally invasive surgery allows for a quicker recovery time and less scarring than traditional open surgery.
It’s recommended to request an appointment with NYGSE to obtain an accurate estimate of the cost.
Bowel Resection Surgery
Bowel resection surgery involves removing a portion of the bowel affected by the endometriosis and reattaching the remaining healthy bowel.
This surgery may be necessary if the endometriosis has caused significant damage to the bowel or if the affected area is too large to be removed by excision alone. In some cases, a temporary colostomy may be needed to allow the bowel to heal properly.
Your doctor will help determine the most appropriate surgical treatment for your individual case of bowel endometriosis.
Robotic-Assisted Surgery
Robotic-assisted surgery is an advanced surgical technique used to treat bowel endometriosis. This technique uses robotic arms controlled by the surgeon to perform the surgery with greater precision and control. The surgeon makes small incisions and inserts the robotic arms and a camera to visualize the surgical field. The surgeon then uses a console to control the robotic arms and perform the surgery.
Robotic surgery is beneficial for bowel endometriosis as it allows the surgeon to make precise and delicate movements, which can be particularly important when working in the delicate tissues of the bowel. It also results in less scarring and pain, a shorter hospital stay, and faster recovery times compared to traditional open surgery. However, not all patients are suitable for robotic surgery, and the decision to use this technique depends on several factors, including the location and severity of the endometriosis.
Service Areas
NYGSE treats women throughout Babylon and Bay Shore, NY with bowel endometriosis, focusing on precise diagnosis and individualized treatment plans that address both pelvic symptoms and gastrointestinal involvement.
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Have Questions About Your Surgery or Treatment?
Expert treatment. Compassionate care. Real results.
November 17, 2025by admin
Pelvic Endometriosis
Understanding Pelvic Endometriosis
Pelvic endometriosis occurs when endometrial-like tissue grows outside the uterus and attaches to structures within the pelvis. Because these implants respond to hormones, they can cause inflammation, scarring, and a wide range of symptoms that often interfere with daily life. Many patients experience painful periods, pelvic pain, pain with intercourse, bowel or bladder discomfort, and in some cases, difficulty becoming pregnant. Pelvic endometriosis can appear in different forms and in different locations, which is why diagnosis and treatment must be tailored to each patient’s needs.
COMMON QUESTIONS ABOUT Pelvic Endometriosis
What are the Causes of Pelvic Endometriosis?
The exact cause of pelvic endometriosis is not fully understood, but there are several theories that attempt to explain its development. Some of the possible factors that may contribute to the development of pelvic endometriosis include:
- Retrograde menstruation: This occurs when menstrual blood flows back through the fallopian tubes and into the pelvic cavity, carrying endometrial cells with it.
- Genetics: Endometriosis tends to run in families, suggesting that there may be a genetic component to its development.
- Immune dysfunction: Some researchers believe that a malfunctioning immune system may be responsible for allowing endometrial tissue to grow outside of the uterus.
- Environmental factors: Exposure to environmental toxins, such as dioxins, may increase the risk of developing endometriosis.
- Hormonal imbalances: Hormonal imbalances, particularly high levels of estrogen, may contribute to the growth and spread of endometrial tissue outside of the uterus.
While the exact cause of pelvic endometriosis remains unclear, it is likely that a combination of these and other factors contribute to its development. Ongoing research is needed to fully understand the causes of this condition and to develop more effective treatment options.
What are the Types of Pelvic Endometriosis?
Pelvic endometriosis can be classified into several different types based on the location and severity of the endometrial tissue growth. Some of the common types of pelvic endometriosis include:
- Superficial endometriosis: This type of endometriosis involves the growth of endometrial tissue on the surface of organs in the pelvis, such as the ovaries, uterus, and fallopian tubes.
- Deep endometriosis: This type of endometriosis occurs when endometrial tissue penetrates deeper into the affected organs or tissues. It can be more difficult to diagnose and treat than superficial endometriosis.
- Ovarian endometriomas: Also known as “chocolate cysts,” these are fluid-filled cysts that form on the ovaries due to the growth of endometrial tissue.
- Adenomyosis: This is a type of endometriosis that occurs when endometrial tissue grows within the muscle walls of the uterus, causing the uterus to become enlarged and painful.
- Bowel endometriosis: This occurs when endometrial tissue grows on or within the walls of the bowel, causing symptoms such as painful bowel movements, diarrhea, and constipation.
Peritoneal Endometriosis
Peritoneal endometriosis is a type of endometriosis that involves the growth of endometrial tissue on the lining of the abdominal cavity, known as the peritoneum. The peritoneum is a thin layer of tissue that covers the abdominal organs and lines the inside of the abdomen.
Peritoneal endometriosis is a common form of endometriosis, and its symptoms can vary from mild to severe. Some of the common symptoms associated with peritoneal endometriosis include painful periods, chronic pelvic pain, pain during intercourse, and infertility.
Diagnosis of peritoneal endometriosis often involves a combination of physical examination, imaging studies (such as ultrasound or MRI), and laparoscopy, which is a minimally invasive surgical procedure that allows a doctor to examine the pelvic organs and tissue for signs of endometriosis.
Treatment for peritoneal endometriosis may include pain management with medications, hormonal therapies to slow the growth of endometrial tissue, or surgery to remove the affected tissue. The specific treatment approach will depend on the severity of the symptoms and the individual needs of each patient.
Rectal Endometriosis
Rectal endometriosis is a type of endometriosis that occurs when endometrial tissue grows on or within the walls of the rectum. The rectum is the final portion of the large intestine, connecting the colon to the anus.
Rectal endometriosis can cause a variety of symptoms, including pain during bowel movements, constipation, diarrhea, abdominal pain, and rectal bleeding. It can also lead to infertility in some cases.
Diagnosis of rectal endometriosis typically involves a combination of physical examination, imaging studies (such as ultrasound or MRI), and sometimes a colonoscopy or proctoscopy to visualize the inside of the rectum.
Ureteral Endometriosis
Ureteral endometriosis is a rare form of endometriosis that occurs when endometrial tissue grows on the ureters, which are the tubes that carry urine from the kidneys to the bladder. This can cause obstruction or narrowing of the ureter, leading to problems with urinary flow and potentially causing kidney damage.
Symptoms of ureteral endometriosis can include pain during urination, blood in the urine, frequent urination, or a urinary tract infection. However, in some cases, there may be no symptoms present.
Diagnosis of ureteral endometriosis may involve imaging studies such as ultrasound or MRI, as well as a specialized diagnostic procedure called a ureteroscopy, which allows a doctor to visualize the inside of the ureter.
Treatment for ureteral endometriosis typically involves surgery to remove the affected tissue and restore normal urinary flow. In some cases, stents or other devices may be used to keep the ureter open during the healing process.
Early detection and treatment of ureteral endometriosis is important to prevent potential complications such as kidney damage.
Bladder Endometriosis
Bladder endometriosis is a type of endometriosis that occurs when endometrial tissue grows on or within the walls of the bladder. The bladder is a hollow organ in the lower abdomen that stores urine.
Symptoms of bladder endometriosis can include painful urination, frequent urination, blood in the urine, or pelvic pain. However, in some cases, there may be no symptoms present.
Diagnosis of bladder endometriosis may involve a physical exam, imaging studies such as ultrasound or MRI, and cystoscopy, which involves inserting a thin, flexible tube with a camera into the bladder to visualize the inside.
Treatment for bladder endometriosis typically involves a combination of medication and surgery. Hormonal treatments, such as birth control pills or GnRH agonists, can help control the growth of endometrial tissue and reduce symptoms. Surgery may be necessary to remove the affected tissue and restore normal bladder function.
How is Pelvic Endometriosis Diagnosed?
Diagnosing pelvic endometriosis can be challenging because its symptoms can be similar to other conditions, such as pelvic inflammatory disease or irritable bowel syndrome. However, there are several methods that healthcare providers may use to diagnose pelvic endometriosis, including:
- Pelvic exam: A pelvic exam can help identify any lumps or abnormalities in the reproductive organs.
- Ultrasound: An ultrasound can help identify the presence of endometriomas or other cysts in the pelvic area.
- Magnetic resonance imaging (MRI): MRI scans can help identify the location and extent of endometriosis tissue.
- Laparoscopy: Laparoscopy is considered the most definitive diagnostic method for pelvic endometriosis. During this procedure, a surgeon inserts a thin, lighted tube (laparoscope) into the abdomen through a small incision. The surgeon can visualize the pelvic organs and take tissue samples for biopsy.
- Blood tests: While there is no specific blood test to diagnose endometriosis, healthcare providers may order blood tests to rule out other conditions.
It is important to note that a definitive diagnosis of pelvic endometriosis can only be made through laparoscopy and tissue biopsy.
Service Areas
At NYGSE, we provide specialized pelvic endometriosis treatment for patients in Babylon, Bay Shore, and surrounding Long Island communities.
Surgical Methods for Pelvic Endometriosis Treatment
There are several surgical methods for treating endometriosis, including laparoscopic excision, robotic-assisted laparoscopy, and laparotomy. The specific method used depends on the severity and location of the endometrial tissue, as well as the patient’s overall health and preferences. In general, the goal of surgery for endometriosis is to remove the affected tissue while preserving healthy tissue and organs as much as possible.
Pelvic Laparoscopic Excision
Pelvic laparoscopic excision is a surgical procedure used to treat pelvic endometriosis. It is also known as laparoscopic excision or laparoscopic surgery.
During the procedure, a surgeon makes a small incision in the abdomen and inserts a laparoscope, which is a thin, flexible tube with a camera and light source. The laparoscope allows the surgeon to view the inside of the abdomen and locate the endometrial tissue.
Using specialized instruments, the surgeon carefully removes the endometrial tissue from the affected areas. The goal of the procedure is to completely remove the endometrial tissue and any adhesions (scar tissue) that may have formed.
Pelvic laparoscopic excision is considered to be a minimally invasive procedure, which means it typically involves less pain and a shorter recovery time than traditional open surgery. However, as with any surgical procedure, there are risks involved, such as bleeding, infection, and damage to surrounding organs.
Pelvic laparoscopic excision is typically recommended for individuals with moderate to severe pelvic endometriosis who have not responded to other treatments such as pain management or hormonal therapy. It is important to work with a healthcare provider to determine if pelvic laparoscopic excision is the best course of treatment for your specific needs.
Robotic-Assisted Laparoscopy
Pelvic robotic-assisted laparoscopy, also known as robot-assisted laparoscopic surgery or da Vinci surgery, is a minimally invasive surgical procedure that uses a robotic system to assist the surgeon in performing the surgery.
During the procedure, the surgeon makes several small incisions in the abdomen and inserts robotic arms and a camera through the incisions. The surgeon sits at a console and controls the robotic arms, which are equipped with miniature surgical instruments.
The robotic system provides several advantages over traditional laparoscopic surgery, such as increased precision, improved visualization, and greater range of motion for the surgical instruments. These benefits can result in a shorter recovery time and less pain for the patient.
However, it is important to note that pelvic robotic-assisted laparoscopy is not appropriate for all cases of pelvic endometriosis. The decision to use robotic-assisted surgery should be made on a case-by-case basis by the healthcare provider and surgeon.
Pelvic Laparotomy
Pelvic laparotomy is a surgical procedure that involves making an incision in the abdomen and pelvic area to gain access to the reproductive organs and surrounding structures. This procedure may be performed to diagnose and treat a variety of gynecologic conditions, including pelvic masses, endometriosis, and ovarian cysts. It is typically reserved for cases where less invasive treatments have been ineffective or are not feasible. Recovery from pelvic laparotomy may take several weeks, and patients are typically advised to avoid strenuous activity during this time.
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Have Questions About Your Surgery or Treatment?
Expert treatment. Compassionate care. Real results.
November 17, 2025by admin
Bladder Endometriosis
Understanding Bladder Endometriosis
Bladder endometriosis occurs when endometrial-like tissue grows on or within the bladder, leading to inflammation, irritation, and urinary symptoms. While less common than pelvic or ovarian endometriosis, it can cause significant discomfort and may affect daily bladder function. Symptoms often overlap with other urologic conditions, which is why accurate diagnosis and individualized treatment are essential. Below is an overview of the causes, symptoms, types, and treatment options for bladder endometriosis.
This illustration shows how endometriosis can develop along the bladder and surrounding pelvic structures. Endometrial-like tissue may implant on the bladder surface or invade deeper layers, leading to inflammation, pain, and urinary symptoms. Understanding where these lesions form helps guide accurate diagnosis and treatment.
COMMON QUESTIONS ABOUT Bladder Endometriosis
What are the Causes of Bladder Endometriosis?
The exact cause of bladder endometriosis is not fully understood, but there are several theories and factors that may contribute to its development. Here are some possible causes and factors associated with bladder endometriosis:
- Retrograde menstruation: Retrograde menstruation is a common theory to explain the development of endometriosis. It occurs when menstrual blood containing endometrial cells flows backward through the fallopian tubes into the pelvic cavity instead of leaving the body. These displaced endometrial cells can attach and grow on the bladder or other pelvic organs.
- Implantation theory: According to this theory, endometrial tissue can be transported to the bladder through the blood or lymphatic system. This may lead to the implantation and growth of endometrial cells on the bladder.
- Metaplasia: Metaplasia refers to the transformation of one type of tissue into another. It is suggested that metaplastic changes in the cells lining the bladder may cause them to transform into endometrial-like cells, leading to bladder endometriosis.
- Surgical scars: Previous surgeries in the pelvic area, such as cesarean sections or hysterectomies, may provide sites for endometrial cells to implant and grow outside the uterus, including on the bladder.
- Genetic factors: There may be a genetic predisposition to developing endometriosis. If a close female relative, such as a mother or sister, has endometriosis, the risk of developing the condition may be higher.
- Hormonal factors: Hormones, especially estrogen, play a crucial role in the development and growth of endometriosis. Hormonal imbalances or abnormalities may contribute to the development of bladder endometriosis.
- Immune system dysfunction: An impaired immune response or dysfunction of the immune system may affect the body’s ability to recognize and eliminate ectopic endometrial cells. This can lead to their attachment and growth in the bladder.
It’s important to note that while these factors are associated with bladder endometriosis, the exact cause can vary from person to person. The condition is still not fully understood, and further research is needed to fully elucidate the underlying causes and mechanisms.
What are the Symptoms of Bladder Endometriosis?
The symptoms of bladder endometriosis can vary from person to person, but here are some common symptoms that individuals may experience:
- Bladder pain: This is one of the primary symptoms of bladder endometriosis. The pain may be experienced as a dull ache, sharp pain, or cramping sensation in the bladder region. The pain can worsen during the menstrual cycle or during bladder filling and may improve after emptying the bladder.
- Urinary frequency: Feeling the need to urinate more often than usual is a common symptom. Individuals with bladder endometriosis may experience increased urinary frequency, even with small amounts of urine.
- Urgency: A sudden and compelling urge to urinate can occur with bladder endometriosis. This sensation may be difficult to control, and individuals may feel the need to rush to the bathroom.
- Painful urination: Some individuals with bladder endometriosis may experience pain or discomfort during urination, known as dysuria. This can be a burning sensation or sharp pain in the urethra or bladder area.
- Blood in the urine: In rare cases, bladder endometriosis can cause bleeding within the bladder, leading to the presence of blood in the urine (hematuria). This symptom should always be evaluated by a healthcare professional to determine its cause.
- Pelvic pain: Bladder endometriosis can cause pelvic pain that may radiate to the bladder region. The pain may be chronic or cyclic, worsening during menstruation.
It’s important to note that these symptoms can also be associated with other urological conditions. If you experience any of these symptoms or suspect bladder endometriosis, it is recommended to consult with a healthcare professional specializing in endometriosis or urology for an accurate diagnosis and appropriate management.
What are the Different Types of Bladder Endometriosis?
Bladder endometriosis is a specific form of endometriosis where endometrial tissue grows and affects the bladder. There are two primary types of bladder endometriosis:
- Superficial Bladder Endometriosis: Superficial bladder endometriosis refers to the presence of endometrial implants on the surface of the bladder. These implants can range in size and may be scattered across the bladder lining. Superficial bladder endometriosis typically affects the mucosal layer of the bladder.
- Bladder Endometriosis Infiltrating the Bladder Wall: In this type, the endometrial tissue infiltrates and penetrates the muscular wall of the bladder. It may extend beyond the mucosal layer and invade the deeper layers of the bladder. This infiltration can cause structural changes and may lead to the formation of fibrotic nodules or adhesions.
Bladder endometriosis can also present in combination with other forms of endometriosis affecting nearby organs in the pelvic region. For example, it can coexist with endometriosis of the uterus, ovaries, fallopian tubes, or other surrounding structures.
It’s important to note that bladder endometriosis is a relatively rare form of endometriosis, with estimates suggesting it occurs in approximately 1-2% of women with endometriosis (Mettler, 2006).
How is Bladder Endometriosis Diagnosed?
The diagnosis of bladder endometriosis typically involves a combination of medical history evaluation, physical examination, imaging studies, and sometimes surgical intervention. Here are the main steps and methods used in the diagnosis of bladder endometriosis:
- Medical history and symptom evaluation: Your healthcare provider will discuss your symptoms, including any pelvic pain, urinary symptoms, or abnormal menstrual cycles. They will inquire about your medical history, including any previous diagnosis or treatment for endometriosis.
- Physical examination: A pelvic examination may be performed to assess for any abnormalities, tenderness, or masses in the pelvic region. However, bladder endometriosis may not be detected through a physical examination alone.
- Imaging studies:
- Ultrasound: Transvaginal ultrasound or pelvic ultrasound may be used to visualize the pelvic organs, including the bladder, and detect any abnormalities or signs of endometriosis.
- Magnetic Resonance Imaging (MRI): An MRI may be recommended to obtain detailed images of the pelvic region. MRI can help identify endometrial lesions and their involvement with the bladder or adjacent structures.
- Cystoscopy: Cystoscopy is a procedure in which a thin, flexible tube with a camera (cystoscope) is inserted into the urethra and advanced into the bladder. This allows for direct visualization of the bladder and the identification of any endometrial implants or lesions on the bladder wall. If suspicious lesions are found, a biopsy may be performed to confirm the presence of endometrial tissue.
- Surgical exploration: In some cases, surgical exploration and excision of suspected endometrial lesions may be necessary for a definitive diagnosis. This may be performed through laparoscopy, a minimally invasive surgical procedure, where a camera and surgical instruments are inserted through small incisions in the abdomen. If bladder endometriosis is confirmed during surgery, excision or ablation of the lesions may be performed.
It’s important to consult with a healthcare professional who specializes in endometriosis or urology for an accurate diagnosis. They will guide you through the appropriate diagnostic steps based on your symptoms, medical history, and physical examination findings.
Service Areas
At NYGSE, we provide specialized bladder endometriosis treatment for patients in Babylon, Bay Shore, and surrounding Long Island communities.
Surgical Methods for Bladder Endometriosis Treatment
Surgical treatment is often required to manage bladder endometriosis effectively. Here are some surgical methods commonly used for bladder endometriosis treatment:
Transurethral Resection of Bladder Endometriosis (TURBE)
This procedure involves using a cystoscope (a thin, flexible tube with a camera) inserted through the urethra to visualize and remove endometrial implants on the bladder wall. It is a minimally invasive procedure and is suitable for smaller lesions or superficial involvement of the bladder.
Since healthcare costs can change over time and vary between different regions, it is difficult to provide an exact figure for the cost of TURBE in the United States. To get an accurate cost estimate, it is advisable to request an appointment with New York Gynecology Surgery & Endometriosis (NYGSE).This procedure involves using a cystoscope (a thin, flexible tube with a camera) inserted through the urethra to visualize and remove endometrial implants on the bladder wall. It is a minimally invasive procedure and is suitable for smaller lesions or superficial involvement of the bladder.
Since healthcare costs can change over time and vary between different regions, it is difficult to provide an exact figure for the cost of TURBE in the United States. To get an accurate cost estimate, it is advisable to request an appointment with NYGSE.
Robotic-Assisted Laparoscopy
Robotic-assisted laparoscopy, also known as robotic-assisted bladder surgery, is a surgical technique that combines laparoscopic surgery with robotic technology to treat bladder endometriosis. This involves using a robotic platform like the da Vinci Surgical System to assist the surgeon in performing precise and controlled movements during the procedure.
The integration of robotic technology in bladder surgery offers several potential benefits, including improved surgical visualization, enhanced surgical precision, and a lower risk of complications. However, it is important to note that not all cases of bladder endometriosis require robotic assistance, and the decision to use robotic-assisted laparoscopy depends on the surgeon’s discretion and the individual patient’s condition.
Laparoscopic Excision
Laparoscopic excision is a minimally invasive surgical technique that involves making small incisions in the abdomen and inserting a laparoscope, which is a thin tube with a camera and surgical instruments. The surgeon uses the laparoscope to visualize and remove the endometrial lesions from the bladder wall. This method is effective for both superficial and deep lesions.
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Have Questions About Your Surgery or Treatment?
Expert treatment. Compassionate care. Real results.
November 11, 2025by admin
Cervical Cancer
Understanding Cervical Cancer
Cervical cancer develops in the cells of the cervix—the lower part of the uterus that connects to the vagina. It is most often caused by long-term infection with certain types of human papillomavirus (HPV), a common sexually transmitted virus. Although it can affect women of any age, it most frequently occurs in women over 30. Regular screenings and HPV vaccination have made cervical cancer one of the most preventable forms of cancer, and when detected early, it is highly treatable.
At New York Gynecology Surgery & Endometriosis (NYGSE), we specialize in the prevention, diagnosis, and treatment of cervical and other gynecologic cancers. Our physicians use advanced technology and a patient-centered approach to provide precise care—from early detection to advanced treatment—helping each woman feel informed, supported, and empowered every step of the way.
COMMON QUESTIONS ABOUT Cervical Cancer
What is Cervical Cancer?
Cancer is a condition characterized by the abnormal growth and multiplication of cells in the body. The name of the cancer is usually derived from the body part where it originates, regardless of whether it later spreads to other areas of the body. In the case of cancer starting in the cervix, it is referred to as cervical cancer. The cervix is the connecting passage between the vagina (birth canal) and the upper part of the uterus, which is where a fetus develops during pregnancy.
All women, irrespective of their age, are susceptible to cervical cancer, though it occurs more frequently in women aged 30 and above. Cervical cancer is primarily caused by a prolonged infection with specific types of human papillomavirus (HPV), a common virus transmitted during sexual activity. Although roughly half of sexually active individuals acquire HPV at some point in their lives, few women develop cervical cancer.
Regular screening tests and HPV vaccination can aid in preventing cervical cancer. If detected early, cervical cancer is highly curable and linked with extended survival and a good quality of life.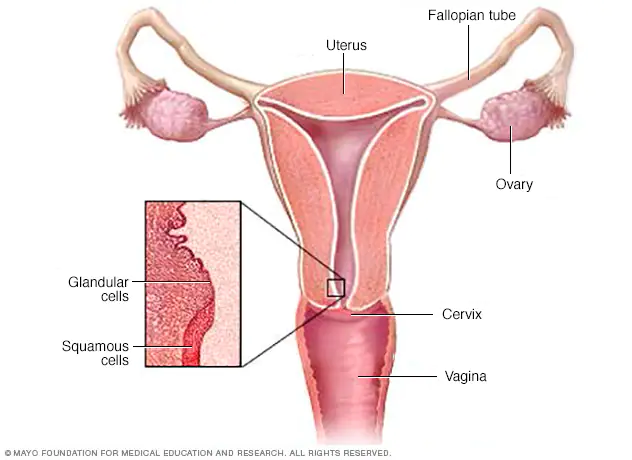
The cervix is the lower, narrow part of the uterus that connects the uterus to the vagina. It is composed of several different parts, including:
- External os: This is the opening of the cervix that faces downward into the vagina.
- Internal os: This is the opening of the cervix that faces upward into the uterus.
- Endocervical canal: This is the passage that runs through the center of the cervix and connects the internal and external os.
- Transformation zone: This is the area of the cervix where the squamous epithelial cells (from the vagina) and columnar epithelial cells (from the uterus) meet. This area is most prone to developing precancerous and cancerous changes.
- Cervical stroma: This is the connective tissue that makes up the bulk of the cervix and contains blood vessels, lymphatic vessels, and nerves.
Understanding the different parts of the cervix is important for screening and diagnosing cervical cancer, as well as for planning treatment.
What are the Different Types of Cervical Cancer?
There are several types of cervical cancer, which are classified based on the type of cell where the cancer originates. The two most common types of cervical cancer are:
- Squamous cell carcinoma: This type of cancer begins in the thin, flat cells that line the outer part of the cervix. Squamous cell carcinoma accounts for about 80-90% of all cervical cancers.
- Adenocarcinoma: This type of cancer starts in the glandular cells that line the inside of the cervix. Adenocarcinoma accounts for about 10-20% of all cervical cancers.
There are also some less common types of cervical cancer, including:
- Adenosquamous carcinoma: This is a type of cancer that has features of both squamous cell carcinoma and adenocarcinoma.
- Small cell carcinoma: This is a rare and aggressive type of cervical cancer that begins in the nerve cells.
- Neuroendocrine tumors: These are rare tumors that develop from the hormone-producing cells in the cervix.
- Glassy cell carcinoma: This is an extremely rare and aggressive form of cervical cancer.
Understanding the type of cervical cancer a patient has is essential for determining the best course of treatment. Treatment options will depend on the type and stage of cancer, as well as the patient’s overall health and preferences.
What are the common Symptoms of Cervical Cancer?
In its early stages, cervical cancer often does not cause any noticeable symptoms. However, as the cancer grows and spreads, it can cause a range of symptoms, which may include:
- Abnormal vaginal bleeding: This may include bleeding between periods, after sex, or after menopause.
- Unusual vaginal discharge: This may be watery, thick, or have a foul odor.
- Pain during sex: This may be due to the tumor pressing against the cervix or surrounding tissues.
- Pelvic pain: This may occur in the lower abdomen or back.
- Painful urination: This may be a sign that the tumor has spread to nearby tissues.
- Swelling in one or both legs: This may occur if the cancer has spread to the lymph nodes or other organs.
It is important to note that many of these symptoms can be caused by conditions other than cervical cancer. However, if any of these symptoms persist for more than a few weeks, it is important to see a healthcare provider for an evaluation. Regular cervical cancer screening tests, such as Pap tests and HPV tests, can also help detect the cancer in its early stages, before it causes symptoms.
What are the Causes of Cervical Cancer?
The main cause of cervical cancer is a long-term infection with certain types of the human papillomavirus (HPV). HPV is a common sexually transmitted virus, and most sexually active people will be infected with HPV at some point in their lives. However, in most cases, the body’s immune system will clear the virus without any problems.
In some cases, however, the virus can cause changes in the cells of the cervix, which can lead to cervical cancer over time. Other factors that may increase the risk of cervical cancer include:
- Smoking: Women who smoke are more likely to develop cervical cancer than non-smokers.
- Weakened immune system: Women with weakened immune systems, such as those who have HIV/AIDS or who have had an organ transplant, are at increased risk of cervical cancer.
- Family history: Women with a family history of cervical cancer may be at increased risk.
- Long-term use of birth control pills: Women who have used birth control pills for several years may have a slightly increased risk of cervical cancer.
- Multiple sexual partners: Women who have had multiple sexual partners may be at increased risk of cervical cancer, as they are more likely to be exposed to HPV.
- Having sex at an early age: Women who had sex for the first time at a young age may be at increased risk of cervical cancer.
It is important to note that having one or more of these risk factors does not mean that a woman will definitely develop cervical cancer. However, women with one or more risk factors may benefit from more frequent cervical cancer screening or other preventive measures.
How can I lower my risk of cervical cancer?
There are several steps women can take to lower their chances of getting cervical cancer:
- Get vaccinated: The HPV vaccine can protect against the types of HPV that are most likely to cause cervical cancer. The vaccine is recommended for girls and boys between the ages of 9 and 26.
- Practice safe sex: Using condoms during sex can help reduce the risk of HPV infection.
- Get regular cervical cancer screenings: Women should start getting regular Pap tests at age 21, or earlier if they are sexually active before age 21. Women over age 30 may also consider getting an HPV test along with their Pap test. These tests can help detect any abnormal cells in the cervix before they become cancerous.
- Quit smoking: Women who smoke are more likely to develop cervical cancer than non-smokers. Quitting smoking can help reduce this risk.
- Maintain a healthy diet and exercise regularly: A healthy lifestyle can help support the immune system and reduce the risk of many types of cancer, including cervical cancer.
- Limit the number of sexual partners: Women who have had multiple sexual partners are at increased risk of HPV infection and cervical cancer.
- Practice good hygiene: Women should avoid using douches or other feminine hygiene products, which can disrupt the natural balance of bacteria in the vagina and increase the risk of infection.
By following these steps, women can lower their risk of developing cervical cancer and improve their overall health.
How is Cervical Cancer Detected?
There are two main tests used to detect cervical cancer:
- Pap test: During a Pap test, a healthcare provider collects cells from the cervix using a small brush or spatula. The cells are then sent to a lab to be examined under a microscope for any abnormalities. Pap tests can detect abnormal cells in the cervix before they become cancerous, which can help prevent cervical cancer or catch it at an early stage when it is highly treatable.
- HPV test: An HPV test looks for the presence of HPV in the cells of the cervix. This test may be done in conjunction with a Pap test in women over the age of 30, or as a follow-up to an abnormal Pap test. HPV testing can help identify women who are at increased risk of developing cervical cancer and may need more frequent screening or further testing.
It is important for women to follow the recommended screening guidelines for cervical cancer, which may vary depending on factors such as age, sexual history, and other risk factors. Women who have any symptoms of cervical cancer, such as abnormal vaginal bleeding, unusual discharge, or pelvic pain, should also see their healthcare provider for evaluation. Early detection and treatment are key to improving outcomes for women with cervical cancer.
Pap Test Result
A Pap test result can be either normal or abnormal. If the results are normal, it means that no abnormal cells were found in the sample collected from the cervix. This is good news, but it is important to remember that a normal Pap test does not completely rule out the possibility of cervical cancer or other gynecological problems.
If the results are abnormal, it means that some of the cells collected during the Pap test looked different from normal cells under the microscope. Abnormal Pap test results do not necessarily mean that a woman has cervical cancer, but they may indicate the presence of precancerous or cancerous cells. Further testing or treatment may be necessary, depending on the specific type and severity of the abnormality.
It is important for women to discuss their Pap test results with their healthcare provider and follow any recommended follow-up testing or treatment. Regular Pap tests and follow-up care are key to preventing and detecting cervical cancer at an early stage when it is highly treatable.
HPV Test Result
The HPV test result can be positive or negative.
- A negative result means that you don’t have the type of HPV that can cause cervical cancer, and your doctor may recommend waiting for your next screening test for up to five years.
- A positive result means that you have an HPV type that may be linked to cervical cancer, but it doesn’t mean you have cancer now. Your doctor may recommend further testing to identify the specific HPV type and determine the next steps.
When to Get Screened
The American Cancer Society (ACS) recommends the following guidelines for cervical cancer screening:
- Women should start getting regular Pap tests at age 21.
- Between ages 21 and 29, women should have a Pap test every three years.
- Between ages 30 and 65, women should have a Pap test and HPV test every five years. Alternatively, they may continue to have a Pap test alone every three years.
- Women over age 65 who have had regular screenings with normal results should not be screened for cervical cancer unless they have a history of cervical pre-cancer or cancer, or a weak immune system.
- Women who have had a total hysterectomy (removal of the uterus and cervix) for non-cancerous reasons do not need to be screened for cervical cancer.
However, it is important for women to discuss their individual risk factors and screening recommendations with their healthcare provider, as some women may need more frequent or earlier screening, and some may be able to stop screening after a certain age or if they have had a hysterectomy.
Stages of Cervical Cancer
Cervical cancer is typically staged using the FIGO (International Federation of Gynecology and Obstetrics) system, which takes into account the size of the tumor, how deeply it has invaded nearby tissues, and whether it has spread to lymph nodes or distant parts of the body. The stages of cervical cancer are as follows:
- Stage 0: This stage, also known as carcinoma in situ, refers to abnormal cells that are found only on the surface of the cervix and have not invaded deeper tissues.
- Stage I: The cancer is confined to the cervix and has not spread to other parts of the body. Stage I is divided into two sub-stages:
- Stage IA: The cancer is small and confined to the cervix.
- Stage IB: The cancer has grown larger, but is still confined to the cervix.
- Stage II: The cancer has spread beyond the cervix and into nearby tissues, such as the upper part of the vagina or the tissue around the uterus. Stage II is also divided into two sub-stages:
- Stage IIA: The cancer has invaded nearby tissues, but not to the pelvic wall.
- Stage IIB: The cancer has spread to the pelvic wall.
- Stage III: The cancer has spread to the lower part of the vagina or to the walls of the pelvis, and may be blocking the ureters (the tubes that carry urine from the kidneys to the bladder). Stage III is also divided into two sub-stages:
- Stage IIIA: The cancer has spread to the lower third of the vagina, but not to the pelvic wall.
- Stage IIIB: The cancer has spread to the pelvic wall or is blocking the ureters.
- Stage IV: The cancer has spread to distant parts of the body, such as the lungs, liver, or bones.
The specific stage of cervical cancer is important in determining the most appropriate treatment options and the likelihood of a cure or long-term survival.
Treatment of Cervical Cancer
The treatment of cervical cancer depends on several factors, including the stage of the cancer, the size and location of the tumor, and the woman’s overall health and personal preferences. Treatment options for cervical cancer may include one or a combination of the following:
- Surgery: Surgery may be recommended for early-stage cervical cancer to remove the cancerous tissue. In some cases, a hysterectomy (removal of the uterus) may be necessary. Lymph nodes may also be removed during surgery to determine if the cancer has spread.
- Radiation therapy: Radiation therapy may be used alone or in combination with surgery for treating cervical cancer. It uses high-energy X-rays or other types of radiation to kill cancer cells.
- Chemotherapy: Chemotherapy is a medication-based treatment that uses drugs to kill cancer cells. It may be used in combination with radiation therapy or surgery for cervical cancer treatment.
- Targeted therapy: This treatment is aimed at specific proteins or genes in the cancer cells to stop the growth and spread of cancer cells.
- Palliative care: Palliative care is used to relieve the symptoms and improve the quality of life of women with advanced cervical cancer. This type of care is provided by a team of healthcare professionals, including doctors, nurses, and social workers.
The choice of treatment and the specific approach depend on various factors such as the stage of the cancer, the patient’s general health, the patient’s preferences, and the availability of resources. Treatment is often most effective when cervical cancer is detected and treated in its early stages. Therefore, regular screening tests are important for women to detect the cancer at an early stage when it is most treatable.
NYGSE Approach
At NYGSE, we have a team of expert oncologists who will guide you through your cancer diagnosis and answer any questions you have. We are dedicated to meeting your specific needs and exceeding your expectations. If you or a loved one is experiencing symptoms of cancer, please call us as soon as possible.
We provide specialized cervical cancer treatment for patients in Babylon, Bay Shore, and surrounding Long Island communities.
Types of Gynecologic Cancer
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Have Questions About Your Surgery or Treatment?
Expert treatment. Compassionate care. Real results.
November 11, 2025by admin
Ovarian Cancer
Understanding Ovarian Cancer
Ovarian cancer develops in the tissues of the ovaries, fallopian tubes, or peritoneum—the protective lining of the abdominal cavity. Because it often causes few noticeable symptoms in its early stages, ovarian cancer is sometimes detected only after it has spread, making early awareness and routine gynecologic care especially important. Common warning signs include bloating, abdominal swelling, pelvic pain, and changes in appetite or urinary habits.
At New York Gynecology Surgery & Endometriosis (NYGSE), we specialize in the diagnosis and treatment of ovarian and related gynecologic cancers using advanced surgical and medical techniques. Our team is dedicated to providing expert, compassionate care—helping each patient understand her options and navigate treatment with confidence, clarity, and the highest level of support.
COMMON QUESTIONS ABOUT Ovarian Cancer
What is Ovarian Cancer?
Abnormal cell growth in the body that occurs uncontrollably is referred to as cancer, often named for the area of origin, despite its later spread to other body parts. Ovarian cancer comprises a cluster of diseases that start in the ovaries or the adjacent fallopian tubes and peritoneum. The pelvis houses two ovaries on either side of the uterus, responsible for generating female hormones and eggs. The fallopian tubes, a pair of long, slender tubes alongside the uterus, transport eggs from the ovaries to the uterus. The peritoneum refers to the covering tissue of abdominal organs. 
Early detection is crucial for successful treatment of ovarian cancer. As the disease often presents with signs and symptoms, it is vital to be aware of your body and recognize what is normal for you. While symptoms may not necessarily indicate cancer, it is advisable to consult a healthcare professional to rule out any concerns.
Certain mutations in genes, such as BRCA1 and BRCA2 genes associated with breast cancer susceptibility and Lynch syndrome, can elevate the risk of ovarian cancer.
Ovarian cancer exists in various tumor types and subtypes, with adenocarcinoma being the most common type and serous adenocarcinoma being the most prevalent subtype. Typically, serous adenocarcinomas are high-grade tumors that grow aggressively.
What are the different Types of Ovarian Cancer?
Ovarian cancer affects either one or both ovaries or the adjacent tissue that envelops the abdominal organs.
There are three main types of ovarian cancer, classified based on the cells where the cancer begins. These include:
- Epithelial ovarian cancer: This type of ovarian cancer begins in the cells that cover the surface of the ovary. Epithelial ovarian cancer is the most common type of ovarian cancer and is responsible for around 90% of cases.
- Germ cell tumors: Germ cell tumors develop in the cells that produce eggs in the ovary. This type of ovarian cancer is rare, accounting for about 5% of cases.
- Stromal tumors: Stromal tumors start in the cells that produce hormones in the ovary. These tumors are also rare and account for about 5% of cases.
Each of these types of ovarian cancer can have different subtypes, which may be classified based on factors such as cell structure, genetic mutations, and growth patterns. The subtype of ovarian cancer can affect how it is treated and the prognosis for the patient.
What are the Symptoms of Ovarian Cancer?
Ovarian cancer can cause a range of symptoms, which may vary depending on the stage and type of cancer. Some of the most common symptoms of ovarian cancer include:
- Bloating or abdominal swelling
- Pelvic pain or pressure
- Difficulty eating or feeling full quickly
- Urinary urgency or frequency
- Back pain
- Fatigue
- Indigestion or heartburn
- Changes in bowel habits, such as constipation or diarrhea
- Menstrual irregularities
- Pain during sexual intercourse
Being attentive to your body and identifying what is usual for you is important. If you experience abnormal vaginal bleeding, it is crucial to seek medical attention immediately. Similarly, if you encounter any of the other symptoms for two weeks or more and they are not typical for you, it is advisable to visit a doctor. Although these symptoms may not necessarily be an indication of cancer, seeking medical attention is the only way to confirm.
What are the most common Causes of Ovarian Cancer?
The exact cause of ovarian cancer is not yet known, but there are several risk factors that may increase the likelihood of developing the disease. These include:
- Age: The risk of ovarian cancer increases as women get older, with most cases occurring in women over age 50.
- Family history: Women with a family history of ovarian cancer, as well as breast and colorectal cancer, are at higher risk. Inherited mutations in the BRCA1 and BRCA2 genes, as well as Lynch syndrome, are also associated with an increased risk of ovarian cancer.
- Reproductive history: Women who have never been pregnant or who had their first pregnancy at an older age may be at higher risk. Starting menstrual periods at a young age or entering menopause at a later age may also increase the risk.
- Hormone therapy: Long-term use of estrogen hormone therapy without progesterone may increase the risk of ovarian cancer.
- Obesity: Obesity may increase the risk of ovarian cancer, particularly in women who have never used hormone therapy.
- Endometriosis: Women with endometriosis, a condition in which the tissue that lines the uterus grows outside the uterus, may be at higher risk.
It’s important to note that having one or more of these risk factors does not necessarily mean a person will develop ovarian cancer. Many women who develop ovarian cancer have no known risk factors, and not all women with risk factors will develop the disease.
How Can I Lower My Chance of Getting Ovarian Cancer?
Although there is no definitive way to prevent ovarian cancer, certain factors have been associated with a decreased risk of developing the disease. These include:
- Using birth control pills for five or more years
- Undergoing a tubal ligation, both ovaries removal, or a hysterectomy
- Giving birth
- Breastfeeding for a year or longer
It is important to consult your doctor to discuss methods of reducing your risk. While these methods may help to lower the risk of ovarian cancer, they are not suitable for everyone, and each one has associated risks and benefits. For example, using birth control pills may increase the risk of developing breast cancer. While it may be possible to lower your risk, there is no guarantee that you will not develop cancer.
How is Ovarian Cancer Detected?
Screening tests and exams are designed to detect a disease in individuals who are not experiencing any symptoms.
Numerous studies have been conducted to create a screening test for ovarian cancer, but they have not been very successful thus far. The two most commonly used screening tests, in addition to a complete pelvic exam, for ovarian cancer are transvaginal ultrasound (TVUS) and the CA-125 blood test.
- Transvaginal ultrasound (TVUS) is a diagnostic tool that employs sound waves to examine the uterus, fallopian tubes, and ovaries by inserting an ultrasound wand into the vagina. Although it can detect a mass (tumor) in the ovary, it cannot determine whether a mass is benign or cancerous. When used for screening purposes, most of the masses discovered are not cancerous.
- The CA-125 blood test measures the amount of a protein known as CA-125 in the blood. Numerous women with ovarian cancer have elevated levels of CA-125. This test can be helpful as a tumor marker to assist in treatment decisions for women who have been diagnosed with ovarian cancer since elevated levels often decrease if the treatment is effective. However, checking CA-125 levels has not been found to be as effective as a screening test for ovarian cancer. The difficulty in using this test for ovarian cancer screening is that high CA-125 levels are often caused by typical conditions such as endometriosis and pelvic inflammatory disease. Furthermore, not all individuals who have ovarian cancer have a high CA-125 level. When an individual who does not have ovarian cancer has an abnormal CA-125 level, the doctor may repeat the test (to verify the result) and may order a transvaginal ultrasound test.
What are the different Stages of Ovarian Cancer?
Ovarian cancer is staged based on the extent of the cancer’s spread within the pelvis and abdomen. The stages of ovarian cancer are:
- Stage I: The cancer is limited to one or both ovaries.
- Stage II: The cancer has spread to other organs within the pelvis, such as the fallopian tubes or uterus.
- Stage III: The cancer has spread beyond the pelvis to the lining of the abdomen and/or nearby lymph nodes.
- Stage IV: The cancer has spread to distant organs, such as the liver or lungs.
Within each stage, there may be further subdivisions based on the extent of the cancer’s spread. The stage of the cancer is an important factor in determining treatment options and prognosis.
Treatment of Ovarian Cancer
The treatment of ovarian cancer depends on several factors, including the stage of the cancer, the type and subtype of ovarian cancer, the woman’s age and overall health, and whether she wants to have children in the future. The main treatments for ovarian cancer include surgery, chemotherapy, and radiation therapy.
- Surgery is often the first treatment for ovarian cancer. The surgeon will remove as much of the cancer as possible, including the ovaries, uterus, fallopian tubes, lymph nodes, and any other tissues that may contain cancer cells. In some cases, the surgeon may recommend a minimally invasive surgery, such as a laparoscopy or a robotic-assisted surgery.
- Chemotherapy is a type of cancer treatment that uses drugs to kill cancer cells. It is usually given after surgery to destroy any remaining cancer cells. Chemotherapy can be given intravenously (through a vein) or directly into the abdomen (intraperitoneal chemotherapy).
- Radiation therapy uses high-energy radiation to kill cancer cells. It is not usually used as the main treatment for ovarian cancer, but it may be used in combination with surgery and chemotherapy in certain cases.
- Targeted therapy is a newer type of cancer treatment that uses drugs to target specific molecules or proteins that are involved in the growth and spread of cancer cells. Targeted therapy is sometimes used in combination with chemotherapy for the treatment of ovarian cancer.
- Immunotherapy is another type of cancer treatment that uses the body’s immune system to fight cancer cells. It is currently being studied for the treatment of ovarian cancer and may be used in the future as a part of a combination therapy.
Overall, the treatment of ovarian cancer is complex and requires a multidisciplinary approach involving a gynecologic oncologist, medical oncologist, radiation oncologist, and other healthcare professionals. The goal of treatment is to cure the cancer or to control its growth and spread, while also preserving the woman’s quality of life.
NYGSE Approach
We understand that an ovarian cancer diagnosis can be overwhelming and scary. Here at NYGSE, we build our teams around you. Our expert oncologists will help guide you through this difficult time, answering any questions you may have along the way. We are here for you and will do everything in our power to meet your specific needs and exceed your expectations.
We provide advanced ovarian cancer treatment for patients in Babylon, Bay Shore, and surrounding Long Island communities.
If you or a loved one is experiencing symptoms that may be related to cancer, please call us as soon as possible.
Types of Gynecologic Cancer
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Have Questions About Your Surgery or Treatment?
Expert treatment. Compassionate care. Real results.
November 11, 2025by admin
Uterine Cancer
Understanding Uterine Cancer
Uterine cancer, also known as endometrial cancer, begins in the lining of the uterus—the organ where a baby grows during pregnancy. It is the most common type of gynecologic cancer in the United States, primarily affecting women after menopause. While abnormal vaginal bleeding is the most common early symptom, uterine cancer can often be detected and treated successfully when caught in its earliest stages.
At New York Gynecology Surgery & Endometriosis (NYGSE), our team provides advanced, individualized care for women diagnosed with uterine and endometrial cancers. Combining surgical expertise, precision diagnostics, and a compassionate approach, we help each patient understand her options and move forward with clarity, confidence, and support.
COMMON QUESTIONS ABOUT Uterine Cancer
What is Uterine Cancer?
Cancer is a disease characterized by uncontrolled cell growth in the body. Typically, cancer is named based on the part of the body where it originates, even if it spreads to other parts later.
Uterine cancer, also known as endometrial cancer, occurs when cancer cells start growing in the uterus. The uterus is a pear-shaped organ located in a woman’s pelvis between the hip bones, where a developing fetus grows during pregnancy.
Endometrial cancer is the most common type of uterine cancer, as it develops in the lining of the uterus known as the endometrium. Although all women with a uterus are at risk for uterine cancer, the risk tends to increase with age, and most cases are diagnosed in women who have already gone through or are going through menopause, which marks the end of menstruation.
The American Cancer Society (ACS) predicts that approximately 65,950 new cases of uterine cancer will be detected in the United States in 2022, with postmenopausal women being the most commonly affected. The average age at which this cancer is usually diagnosed is 60.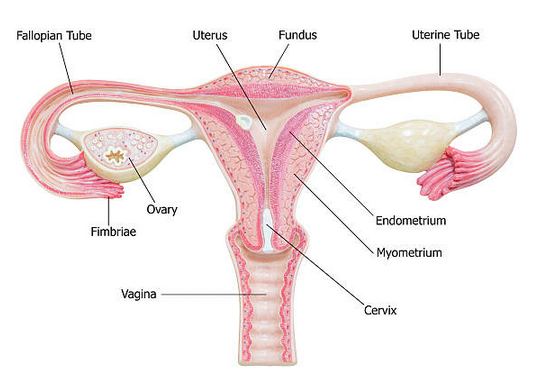
What are the different Types of Uterine Cancer?
Uterine cancer has two primary types that develop in different parts of the uterus:
- Endometrial cancer: This is the most common type of uterine cancer, accounting for more than 90% of cases. It starts in the cells of the endometrium, which is the lining of the uterus.
- Uterine sarcoma: This is a less common type of uterine cancer that starts in the muscle or other tissues of the uterus. It accounts for less than 10% of uterine cancers.
What are the Symptoms of Uterine Cancer?
Abnormal vaginal discharge or bleeding that is unusual for you may be a symptom of uterine cancer. Bleeding may be considered abnormal if it occurs after menopause or between periods, or if it is heavier than usual. It’s important to note that bleeding after periods have stopped is never considered normal. Uterine cancer may also cause pelvic pain or pressure.
If you experience abnormal bleeding, particularly if you have already gone through menopause, it’s crucial to see a doctor immediately. Additionally, if you have any other signs or symptoms that persist for two weeks or more, it’s important to seek medical attention. While these symptoms could be due to other conditions, the only way to determine the cause is to consult with your doctor.
What are the most common Causes of Uterine Cancer?
Uterine cancer occurs when cells in the uterus grow and multiply abnormally, leading to the formation of a tumor. The exact cause of uterine cancer is unknown, but certain factors have been identified that increase a woman’s risk of developing this disease. These risk factors include:
- Age: The risk of uterine cancer increases as women get older, especially after menopause.
- Hormonal imbalances: An excess of estrogen or a lack of progesterone in the body can increase the risk of uterine cancer.
- Obesity: Being overweight or obese increases the risk of uterine cancer.
- Diabetes: Women with diabetes have a higher risk of developing uterine cancer.
- Family history: Women who have a family history of uterine, ovarian, or colorectal cancer have a higher risk of developing uterine cancer.
- Endometrial hyperplasia: This is a condition where the lining of the uterus grows too thick, which can increase the risk of developing uterine cancer.
- Tamoxifen: This medication, which is used to treat breast cancer, can increase the risk of uterine cancer.
How Can I Lower My Chance of Getting Uterine Cancer?
There are no known methods to completely prevent uterine cancer. However, some factors may lower your risk of developing uterine cancer:
- Using birth control pills.
- Maintaining a healthy weight and being physically active.
- Taking progesterone along with estrogen.
It is advisable to consult your doctor regarding how often you should undergo screening for uterine cancer, particularly if you believe that you have risk factors that increase your chances of getting it. While these measures may aid in reducing the risk of uterine cancer, they are not recommended for everyone and have associated risks and benefits. For instance, birth control pills may increase the risk of breast cancer.
Detection of Uterine Cancer
Uterine cancer can be detected through various tests and procedures. The doctor may perform a pelvic exam to check for any abnormality or growths in the uterus. Imaging tests such as transvaginal ultrasound, CT scan, and MRI can also help detect any abnormal growth or mass in the uterus.
- A biopsy is the most reliable way to diagnose uterine cancer. It involves removing a small piece of tissue from the uterus for examination under a microscope. There are different types of biopsies, including endometrial biopsy, dilation and curettage (D&C), and hysteroscopy.
- An endometrial biopsy is performed in the doctor’s office by inserting a thin, flexible tube through the cervix into the uterus to collect a sample of the endometrial tissue. D&C involves dilating the cervix and scraping the lining of the uterus to collect a tissue sample. Hysteroscopy involves using a thin, lighted tube with a camera to view the inside of the uterus and remove a tissue sample.
- If uterine cancer is diagnosed, additional tests such as a chest X-ray, CT scan, or MRI may be performed to determine the stage and extent of the cancer.
What are the Stages of Uterine Cancer?
The process of determining the location and extent of cancer in the body, as well as whether it has spread and is affecting other parts of the body, is referred to as staging. Diagnostic tests are used by doctors to determine the cancer’s stage, and information based on tissue samples collected during surgery may be required.
Because of this, staging may not be complete until all tests are finished and the tumor has been removed through surgery (see Types of Treatment). Knowing the stage is important as it helps the doctor suggest the most effective treatment and can also assist in predicting the prognosis, or the likelihood of recovery. Different stage descriptions are used for different types of cancer. The staging system used for uterine cancer is the one developed by the International Federation of Obstetrics and Gynecology (FIGO).
The stage provides a common way of describing the cancer, enabling doctors to work together to plan the best treatments. Doctors assign the stage of endometrial cancer using the FIGO system.
Stage I: The cancer is found only in the uterus or womb, and it has not spread to other parts of the body.
- Stage IA: The cancer is found only in the endometrium or less than one-half of the myometrium.
- Stage IB: The tumor has spread to one-half or more of the myometrium.
Stage II: The tumor has spread from the uterus to the cervical stroma but not to other parts of the body.
Stage III: The cancer has spread beyond the uterus, but it is still only in the pelvic area.
- Stage IIIA: The cancer has spread to the serosa of the uterus and/or the tissue of the fallopian tubes and ovaries but not to other parts of the body.
- Stage IIIB: The tumor has spread to the vagina or to the tissue immediately next to the uterus called the parametrium.
- Stage IIIC1: The cancer has spread to the regional pelvic lymph nodes. Lymph nodes are small, bean-shaped organs that help fight infection.
- Stage IIIC2: The cancer has spread to the para-aortic lymph nodes with or without spread to the regional pelvic lymph nodes.
Stage IV: The cancer has metastasized to the rectum, bladder, and/or distant organs.
- Stage IVA: The cancer has spread to the mucosa of the rectum or bladder.
- Stage IVB: The cancer has spread to lymph nodes in the groin area, and/or it has spread to distant organs, such as the bones or lungs.
What is Uterine Cancer Grade?
The medical professionals also classify this form of cancer by its grade (G), which reflects the degree of similarity between cancer cells and healthy cells under a microscope. By examining the cancerous tissue alongside healthy tissue, doctors can determine if the cancer cells have similar cell groupings to healthy cells, which is known as “differentiated” or “low-grade tumor,” or if the cancer cells look significantly different from healthy tissue, which is referred to as “poorly differentiated” or “high-grade tumor.” The grade of cancer may help doctors forecast how rapidly the cancer will develop. In general, a slower growth rate is associated with a more favorable prognosis.
The letter “G” is used to define a grade for uterine cancer.
- GX: The grade cannot be evaluated.
- G1: The cells are well differentiated.
- G2: The cells are moderately differentiated.
- G3: The cells are poorly differentiated.
Treatment of Uterine Cancer
In case you have been diagnosed with uterine cancer, you can request your doctor to refer you to a gynecologic oncologist, a specialist who is trained to treat such cancers. You can work together with this doctor and their team to develop a treatment plan.
What are the different Types of Treatment for Uterine Cancer?
There are several treatment options for uterine cancer, including:
- Surgery: The most common treatment for uterine cancer is surgery to remove the uterus (hysterectomy). The surgeon may also remove the fallopian tubes, ovaries, and nearby lymph nodes. In some cases, a woman may be able to have a minimally invasive surgery instead of an open surgery.
- Radiation therapy: Radiation therapy uses high-energy radiation to kill cancer cells. It can be given externally (from outside the body) or internally (from inside the body).
- Chemotherapy: Chemotherapy is a drug treatment that kills cancer cells. It may be given before surgery to shrink the tumor or after surgery to kill any remaining cancer cells.
- Hormone therapy: Hormone therapy uses drugs to block hormones that may be fueling the growth of cancer cells. This treatment is only used for certain types of uterine cancer.
The choice of treatment depends on the stage of the cancer, the grade of the cancer, the woman’s age and overall health, and other factors. The treatment plan is usually developed by a team of doctors, including a gynecologic oncologist, who specializes in treating cancers of the female reproductive system.
NYGSE Approach
We understand that a cancer diagnosis can be overwhelming and scary. Here at NYGSE, we build our teams around you. Our expert oncologists will help guide you through this difficult time, answering any questions you may have along the way. We are here for you and will do everything in our power to meet your specific needs and exceed your expectations.
If you or a loved one is experiencing symptoms that may be related to cancer, please call us as soon as possible.
We provide advanced uterine cancer treatment for patients in Babylon, Bay Shore, and surrounding Long Island communities.
Types of Gynecologic Cancer
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Have Questions About Your Surgery or Treatment?
Expert treatment. Compassionate care. Real results.
November 11, 2025by admin
Vaginal Cancer
Understanding Vaginal Cancer
Vaginal cancer is a rare form of gynecologic cancer that develops in the tissue lining of the vagina. It accounts for only a small percentage of gynecologic cancers diagnosed each year and often begins as precancerous changes known as vaginal intraepithelial neoplasia (VaIN). Because symptoms can be subtle or absent in early stages, regular gynecologic exams and attention to any unusual bleeding or discharge are key to early detection.
At New York Gynecology Surgery & Endometriosis (NYGSE), our specialists provide advanced diagnosis and treatment for rare gynecologic cancers like vaginal cancer. We combine surgical precision, leading technology, and compassionate care to ensure every patient receives the best possible outcome and ongoing support through treatment and recovery.
COMMON QUESTIONS ABOUT vaginal Cancer
What is Vaginal Cancer?
Cancer is a condition characterized by uncontrolled cell growth within the body. It is typically named after the specific area where it originates, even if it eventually spreads to other parts of the body.
When cancer originates in the vagina, it is referred to as vaginal cancer. The vagina, also known as the birth canal, serves as the passage for menstrual blood and childbirth. It is connected to the cervix, the opening of the uterus, and surrounded by folds of skin known as the vulva.
Under normal circumstances, the vagina remains collapsed with its walls touching. However, during sexual intercourse and vaginal childbirth, the vaginal walls can expand due to numerous folds. The vaginal lining stays moist through mucus released from glands in the cervix.
The vaginal walls consist of a thin layer of cells known as the epithelium, containing squamous epithelial cells. Below the epithelium, the vaginal wall is composed of connective tissue, involuntary muscle tissue, lymph vessels, and nerves.
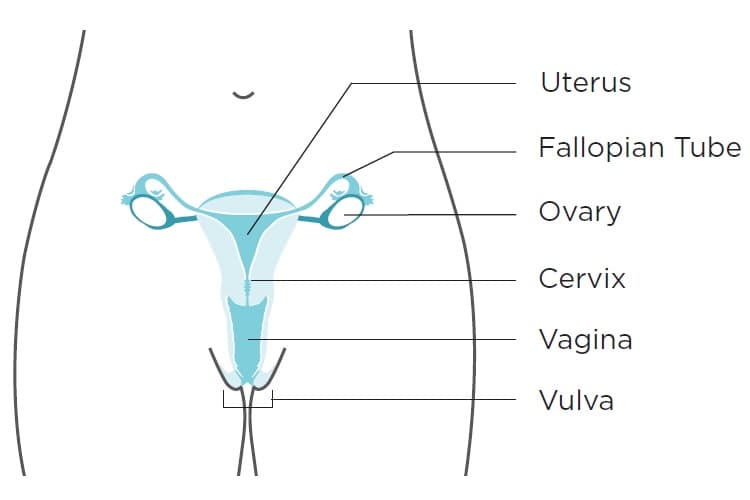 Vaginal cancer is an extremely uncommon occurrence. While all women face some risk of these cancers, the likelihood of developing them is very low. Together, vaginal cancers account for approximately 7% of all gynecologic cancers diagnosed in the U.S.
Vaginal cancer is an extremely uncommon occurrence. While all women face some risk of these cancers, the likelihood of developing them is very low. Together, vaginal cancers account for approximately 7% of all gynecologic cancers diagnosed in the U.S.
Approximately 85% of vaginal cancer cases actually stem from cancer that has spread from other parts of the body, with about half of these originating from the cervix or uterus.
What are the different Types of Cervical Cancer?
The vagina can be affected by five main types of cancer:
- Squamous cell carcinoma: This type of cancer originates in the cells lining the vagina, typically occurring near the cervix. Squamous cell carcinoma constitutes approximately 85% of vaginal cancer cases. Its development is gradual, often beginning with a precancerous condition known as vaginal intraepithelial neoplasia (VaIN), as described earlier.
- Adenocarcinoma: Adenocarcinoma starts in the glandular tissue of the vagina and accounts for about 5% to 10% of vaginal cancers.
- Clear cell adenocarcinoma: This particular cancer is associated with individuals whose mothers were exposed to the drug diethylstilbestrol (DES) during pregnancy between the late 1940s and 1971. It is a rare type of cancer, and it is estimated that approximately 1 in 1,000 people exposed to DES may develop vaginal cancer.
- Melanoma: While rare, melanoma can originate in the vagina. Melanomas typically occur on sun-exposed skin areas, but they can occasionally develop in regions with no sun exposure. They often present as dark-colored lesions with irregular borders.
- Sarcomas: These are uncommon tumors that can begin in the vagina. Several subtypes of sarcomas exist, each with its distinct characteristics.
Understanding the different types of vaginal cancer is crucial for early detection and appropriate treatment.
What are the Symptoms of Vaginal Cancer?
In the early stages, most vaginal cancers do not exhibit noticeable signs or symptoms. However, as the disease progresses, the following signs and symptoms may become apparent:
- Unusual vaginal discharge or abnormal bleeding: This bleeding may differ from your normal menstrual flow, either in terms of heaviness or timing. It could include bleeding after menopause, bleeding between periods, or any bleeding that is unusually prolonged or heavy for your typical pattern.
- Alterations in bathroom habits: You might experience blood in your stool or urine, find yourself using the bathroom more frequently than usual, or encounter constipation.
- Pelvic pain: Discomfort in the pelvic region, which refers to the area below your stomach and between your hip bones, may occur, particularly during urination or sexual intercourse.
As these symptoms can be indicative of vaginal cancer, it is essential to seek medical attention promptly if you experience any of these warning signs. Early detection and treatment can significantly improve the chances of successful outcomes.
What are the Causes of Vaginal Cancer?
Factors that may increase your risk of developing vaginal cancer include:
- Advancing age: As you reach the age of 60 or older, the risk of vaginal cancer tends to increase. The most common type, squamous cell carcinoma, is typically diagnosed around this age.
- Human papillomavirus (HPV) infection: Having HPV, a sexually transmitted virus, can elevate the risk of both cervical and vaginal cancer. Unprotected sexual activity with multiple partners and lack of HPV vaccination further heightens the likelihood of HPV infection.
- Vaginal intraepithelial neoplasia (VAIN): If you have VAIN, which involves abnormal cells in the vaginal lining (but not cancer cells), there is a potential for VAIN to progress to vaginal cancer. However, the reason why this progression occurs in some individuals and not others remains unclear. Having HPV increases the likelihood of developing VAIN.
- History of cervical cancer or cervical dysplasia: Women who have experienced cervical cancer or cervical dysplasia have a possibility of developing vaginal cancer in the future. The presence of abnormal cells in the cervix may contribute to the increased risk.
- Exposure to diethylstilbestrol (DES): DES, a synthetic estrogen prescribed between 1940 and 1971 to prevent pregnancy complications, can raise the risk of developing adenocarcinoma. If your birthing parent took DES during pregnancy, and you were exposed to it, your risk may be increased.
- Smoking: Smoking tobacco can double your risk of developing vaginal cancer.
It is essential to be aware of these risk factors and take necessary precautions, such as regular medical check-ups and lifestyle adjustments, to minimize the likelihood of developing vaginal cancer.
How Can I Lower My Chance of Getting Vaginal Cancer?
While it may not be possible to completely prevent vaginal cancer, there are measures you can take to reduce your risk:
Human papillomavirus (HPV) is a widespread virus consisting of over 200 different types, with more than 30 of them transmitted through close skin-to-skin contact during sexual activity. Most cases of cervical cancer and some instances of vaginal, vulvar, and other cancers are attributed to HPV infections.
The HPV vaccine is an effective way to safeguard against the types of HPV that commonly lead to cervical, vaginal, and vulvar cancers.
Here are the recommended guidelines for HPV vaccination:
- Preteens between the ages of 11 and 12 years should receive the HPV vaccine, with the option to start as early as age 9.
- The HPV vaccine is also recommended for individuals up to the age of 26 years, if they have not been vaccinated previously.
- For those older than 26 years, HPV vaccination is generally not advised. However, some adults aged 27 to 45 years, who have not been vaccinated before, may choose to consult their doctor about their risk of new HPV infections and the potential benefits of vaccination. It’s important to note that HPV vaccination in this age range may offer less protection, as many people might have already been exposed to HPV.
By following these vaccination recommendations and engaging in open discussions with healthcare professionals, you can take proactive steps to reduce the likelihood of HPV-related cancers, including vaginal cancer.
The recommended HPV vaccination schedule depends on the age at which it is initiated. If vaccination begins before reaching the age of 15, a two-dose schedule is advised, with the doses administered 6 to 12 months apart. However, for those who commence the vaccination series after their 15th birthday, a three-shot schedule is given.
It’s important to note that HPV vaccination serves as a preventive measure against new HPV infections, but it does not treat existing infections or diseases. Consequently, the HPV vaccine is most effective when administered before any exposure to HPV occurs. Even if you have received the HPV vaccine, regular screening for cervical cancer is essential to ensure early detection and appropriate management, as the vaccine does not provide protection against existing infections.
How is Vaginal Cancer Detected?
Screening for vaginal cancers in asymptomatic women is currently challenging as there is no simple and reliable test available for this purpose.
Screening involves using tests to detect a disease before any symptoms are evident. Effective cancer screening tests are instrumental in early disease detection, leading to more successful treatment outcomes. Diagnostic tests, on the other hand, are employed when a person exhibits symptoms. Their purpose is to identify the underlying cause of the symptoms. Diagnostic tests may also be conducted on individuals considered at high risk for cancer.
It is essential to recognize that the Pap test, although valuable for cervical cancer screening, does not screen for vaginal cancer. As no straightforward and dependable screening methods exist for most gynecologic cancers, except for cervical cancer, it becomes even more critical to be vigilant for potential warning signs and take measures to lower your risk.
Here are some proactive steps you can take:
- Be attentive to your body and be aware of what is normal for you.
- If you observe any changes in your body that are abnormal for you and could be indicative of vaginal or vulvar cancer, discuss them with your doctor and inquire about possible causes.
- Regularly visit your doctor for checkups. During these checkups, your doctor may perform a pelvic examination to identify signs of vaginal and vulvar cancer.
If a pelvic exam or Pap test raises concerns, your doctor may conduct a colposcopy. This procedure employs a lighted magnifying tool called a colposcope to examine your vagina and cervix for any unusual findings. A small tissue sample, known as a biopsy, might also be taken for further examination under a microscope by a specialist.
Upon diagnosing vaginal cancer, your doctor may order imaging tests and additional examinations to determine whether the cancer has spread to other parts of your body. This helps them establish the stage of the cancer and plan the appropriate treatment approach. Being proactive in monitoring your health and seeking timely medical attention can play a crucial role in detecting and managing vaginal cancer effectively.
What are the Stages of Vaginal Cancer?
Once a woman is diagnosed with vaginal cancer, medical professionals will conduct a process called staging to ascertain whether the cancer has spread and to what extent. Staging involves determining the amount of cancer present in the body, providing crucial information on the severity of the cancer and guiding the most appropriate treatment approach. Additionally, when discussing survival statistics, doctors use the cancer’s stage as a reference.
The stages of vaginal cancer are categorized from stage I (1) to IV (4). Generally, lower numbers indicate less cancer spread, while higher numbers, like stage IV, signify more extensive cancer spread. Although each individual’s experience with cancer is unique, cancers at similar stages tend to have comparable prognoses and are often treated using similar methods.
Both the FIGO (International Federation of Gynecology and Obstetrics) system and the AJCC (American Joint Committee on Cancer TNM staging system) are fundamentally similar when staging vaginal cancer.
They both utilize three key pieces of information to classify the cancer:
- The tumor’s extent (T): This entails assessing the size of the cancer and whether it has invaded the vaginal wall. Furthermore, the evaluation includes determining if the cancer has spread to nearby structures, such as the pelvic wall, which encompasses the internal cavity containing the female reproductive organs, rectum, bladder, and sections of the large intestine.
- The involvement of nearby lymph nodes (N): The staging process involves investigating whether the cancer has extended to the lymph nodes in the pelvic or groin (inguinal) area.
- The presence of distant metastasis (M): The staging evaluation includes determining whether the cancer has spread to distant lymph nodes or organs in the body.
By considering these three critical pieces of information, both staging systems provide a comprehensive assessment of the extent and progression of vaginal cancer, aiding in effective treatment planning and prognosis determination.
The T, N, and M staging components are further detailed by numbers or letters, offering more specific information about each factor. Higher numbers indicate a more advanced stage of cancer. After determining a person’s T, N, and M categories, this data is combined through a process known as stage grouping, resulting in an overall stage classification.
The table’s staging system primarily employs the clinical stage, which is determined based on the results of physical examinations, biopsies, and imaging tests conducted before any surgical procedures. Surgical staging, on the other hand, is established by examining the tissue removed during an operation. For further information on cancer staging, please refer to Cancer Staging.
The following system is the most recent AJCC system, which became effective in January 2018.
It’s important to note that these staging systems are not utilized for staging vaginal melanoma, as melanoma of the skin and vaginal melanoma are staged in a similar manner. For details on melanoma staging, refer to information about Melanoma Skin Cancer.
Given the complexity of vaginal cancer staging, it is advisable to ask your doctor to explain it to you in a manner that you can understand fully. This will ensure that you have a clear grasp of your specific situation and the implications of the staging process.
Stage 1
Stage 1 vaginal cancer indicates that the cancer has begun to grow into the vaginal wall but has not spread beyond that point.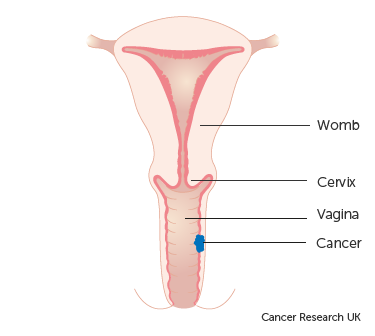
This stage is further divided into two groups:
- Stage 1A: The cancer is localized solely within the vagina and is not larger than 2cm in size. Additionally, it has not spread to nearby lymph nodes close to the vagina.
- Stage 1B: The cancer is confined to the vagina, but it measures more than 2cm in size. Similar to Stage 1A, it has not spread to lymph nodes in the vicinity of the vagina.
Stage 2
This stage is categorized into two groups:
- Stage 2A: In this stage, the cancer has extended beyond the confines of the vagina into the surrounding tissues. However, it has not reached the walls of the pelvis or nearby lymph nodes. Additionally, the size of the cancer is not larger than 2cm.
- Stage 2B: Similar to Stage 2A, the cancer has spread beyond the vagina into the surrounding tissues without reaching the walls of the pelvis or nearby lymph nodes. However, in this case, the size of the cancer is larger than 2cm.
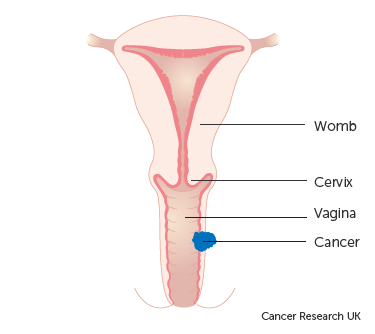
Stage 3
At this stage, the cancer has advanced beyond the vaginal area and infiltrated the side walls of the pelvis. Consequently, this can lead to urinary difficulties, such as experiencing pain or noticing blood during urination. Additionally, cancer cells might be detected in the lymph nodes located near the vagina.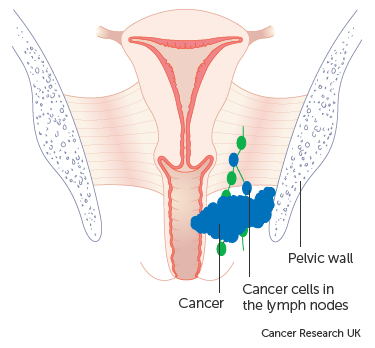
Stage 4
This stage indicates advanced vaginal cancer, signifying that the cancer has metastasized to organs beyond the vagina.
Stage 4 is further divided into two groups:
- Stage 4A: In this group, the cancer has spread to other organs, such as the bladder or rectum (back passage).
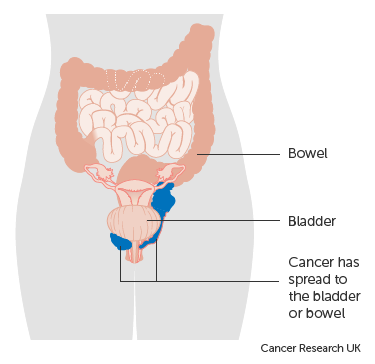
Stage 4B represents an advanced condition where the cancer has extended to distant organs, such as the lungs or bones.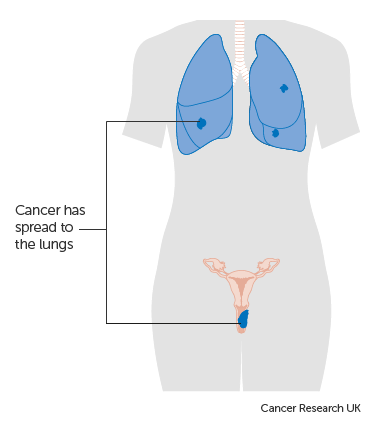
Treatment of Vaginal Cancer
Patients diagnosed with vaginal cancer have access to various treatment options. These treatments can be categorized into standard procedures, which are the currently established therapies, and experimental approaches that are being investigated in clinical trials. Clinical trials are research studies conducted to enhance existing treatments or gather data on novel treatments for cancer patients. If clinical trials demonstrate that a new treatment is more effective than the standard one, it may replace the current standard of care.
Patients may consider participating in clinical trials to contribute to medical advancements. Some trials may only be available to patients who have not yet begun any treatment.
Types of Treatment
Surgery is one of the treatment options for vaginal cancer, and the following surgical procedures may be used:
- Wide local excision: This surgical procedure involves removing the cancer along with some surrounding healthy tissue.
- Vaginectomy: In this surgery, all or part of the vagina is removed. In some cases, skin grafts from other areas of the body may be necessary to reconstruct the vagina.
- Total hysterectomy: This surgery involves the removal of the uterus, including the cervix. Depending on the approach, it can be performed as a vaginal hysterectomy (via the vagina), a total abdominal hysterectomy (through a large incision in the abdomen), or a total laparoscopic hysterectomy (through a small incision in the abdomen using a laparoscope).
- Lymph node dissection: This surgical procedure entails removing lymph nodes, and a tissue sample is examined under a microscope to check for signs of cancer. It is also known as lymphadenectomy. If the cancer is in the upper vagina, pelvic lymph nodes may be removed, while lymph nodes in the groin may be removed if the cancer is in the lower vagina.
- Pelvic exenteration: This extensive surgery involves removing the lower colon, rectum, bladder, cervix, vagina, and ovaries. Nearby lymph nodes are also removed. As a result of this procedure, artificial openings (stoma) are created to allow urine and stool to be collected in external bags.
These surgical options are employed based on the specific characteristics of the vaginal cancer and the patient’s overall health condition. The choice of surgery will be determined in collaboration with the medical team to ensure the most appropriate and effective treatment plan.
Following the surgical removal of all visible cancer, certain patients may receive radiation therapy as a subsequent treatment to eliminate any remaining cancer cells. This post-surgery treatment, aimed at reducing the risk of cancer recurrence, is referred to as adjuvant therapy. Its purpose is to target any residual cancer cells that might not have been removed during the surgery, thereby enhancing the chances of long-term remission.
Radiation therapy
Radiation therapy is a cancer treatment that employs high-energy x-rays or other forms of radiation to either destroy cancer cells or prevent their further growth. There are two main types of radiation therapy:
- External radiation therapy involves utilizing a machine located outside the body to direct radiation towards the specific area of the body affected by cancer.
- Internal radiation therapy, also known as brachytherapy, entails using a sealed radioactive substance, such as needles, seeds, wires, or catheters, which are directly inserted into or placed near the cancer site to administer targeted radiation treatment.
The administration of radiation therapy is tailored to the specific type and stage of the cancer being treated. In the case of vaginal cancer, both external and internal radiation therapies are employed to target the disease effectively. Additionally, these radiation treatments can also serve as palliative therapy to alleviate symptoms and enhance the patient’s overall quality of life.
Chemotherapy is a cancer treatment that employs medications to halt the growth of cancer cells, either by inducing their death or preventing their division. The administration of chemotherapy can be through oral intake or injection into a vein or muscle, which allows the drugs to enter the bloodstream and reach cancer cells throughout the body (systemic chemotherapy). Alternatively, when chemotherapy is directly introduced into the cerebrospinal fluid, an organ, or a body cavity like the abdomen, its effects are primarily targeted at cancer cells in those specific areas (regional chemotherapy). The choice of chemotherapy method is determined based on the type and stage of the cancer being treated.
For squamous cell vaginal cancer, topical chemotherapy may be applied to the vagina using a cream or lotion, providing a localized treatment approach.
New types of treatment are being tested in clinical trials.
The following section provides an overview of treatments currently under investigation in clinical trials. Please note that not all new treatments being studied are mentioned in this summary.
Immunotherapy
Immunotherapy is a cancer treatment method that harnesses the patient’s own immune system to combat cancer. It involves using substances produced by the body or created in a laboratory to enhance, direct, or restore the body’s natural defenses against cancer. This approach is considered a form of biologic therapy.
Imiquimod, an immune response modifier, is currently being researched for its potential in treating vaginal lesions. It is applied to the skin in the form of a cream.
Radiosensitizers
Radiosensitizers are drugs that increase the sensitivity of tumor cells to radiation therapy. Combining radiation therapy with radiosensitizers has the potential to eliminate more tumor cells.
NYGSE Approach
At NYGSE, we acknowledge that a cancer diagnosis can be a daunting and unsettling experience. That’s why we prioritize building teams centered around you. Our dedicated oncologists are here to support and assist you throughout this challenging journey, addressing any concerns or inquiries you may have. You can count on us to provide personalized care that meets your unique requirements and surpasses your expectations.
If you or a loved one are encountering symptoms that could be connected to cancer, we encourage you to contact us at your earliest convenience. We are here to help and offer the best possible care for your well-being.
We provide advanced vaginal cancer treatment for patients in Babylon, Bay Shore, and surrounding Long Island communities.
Types of Gynecologic Cancer
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Have Questions About Your Surgery or Treatment?
Expert treatment. Compassionate care. Real results.
November 10, 2025by admin
Vulvar Cancer
Understanding Vulvar Cancer
Vulvar cancer is a rare form of gynecologic cancer that develops on the outer surface of the female genital area. It can appear as a sore, lump, or patch of skin that changes in color or texture, often accompanied by itching or discomfort. While it can affect women of any age, it is most commonly diagnosed in older adults. Early detection is key—when identified in its initial stages, treatment is often highly successful.
At New York Gynecology Surgery & Endometriosis (NYGSE), our specialists are experienced in diagnosing and treating vulvar cancer with advanced surgical and medical approaches. We focus on providing expert care with sensitivity and precision, helping women understand their condition, explore treatment options, and achieve the best possible outcome with confidence and support.
COMMON QUESTIONS ABOUT Vulvar Cancer
What is Vulvar Cancer?
Vulvar cancer is a form of cancer that develops on the external surface of the female genitalia. The vulva refers to the skin area encircling the urethra and vagina, which includes:
- The lips encompassing the vagina (labia minora and labia majora).
- The clitoris, a sexual organ vital in achieving sexual climax.
- The Bartholin’s glands, two small glands on each side of the vagina.
Typically, vulvar cancer manifests as a lump or sore on the vulva, often accompanied by itching. While it can occur at any age, it is more commonly diagnosed in older adults.
The treatment for vulvar cancer generally involves surgical intervention to remove the cancerous tissue along with a small portion of the surrounding healthy tissue. In some cases, extensive surgery may be necessary, which could involve the removal of the entire vulva. The prognosis and complexity of the surgery tend to improve significantly when vulvar cancer is detected at an early stage.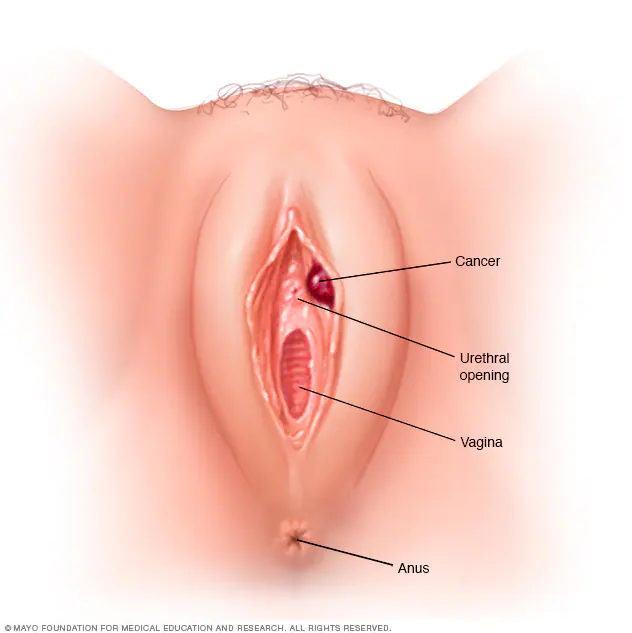 In the United States, approximately 6,000 new cases of vulvar cancer are reported each year. Among these cases, roughly half are attributed to human papillomavirus (HPV), and the other half are associated with lichen sclerosus. Vulvar cancer is considered a highly uncommon form of cancer, making up only 0.6 percent of all cancer diagnoses in women.
In the United States, approximately 6,000 new cases of vulvar cancer are reported each year. Among these cases, roughly half are attributed to human papillomavirus (HPV), and the other half are associated with lichen sclerosus. Vulvar cancer is considered a highly uncommon form of cancer, making up only 0.6 percent of all cancer diagnoses in women.
What are the different Types of Vulvar Cancer?
Vulvar cancer encompasses various types, with squamous cell carcinoma being the most prevalent. Approximately 90% of vulvar cancers are squamous cell carcinomas, mainly found on the labia.
Squamous cell carcinoma can develop from a precancerous condition known as vulva intraepithelial neoplasia (VIN). VIN involves cell changes that may or may not progress to cancer. It is crucial to note that VIN is considered a premalignant growth, meaning it is not yet cancerous. VIN is further categorized into two groups based on cellular appearance under a microscope: “usual-type VIN” typically seen in younger women, associated with human papillomavirus (HPV), and “differentiated VIN,” less common and prevalent in older women, not linked to HPV. Differentiated VIN often occurs in women with lichen sclerosus, a skin condition that is likely to be diagnosed by a gynecologist and may or may not be known prior to VIN. It’s important to be aware that this form of VIN can potentially develop into a fast-moving, aggressive squamous cancer. Refer to Risk Factors and Prevention for more information on HPV, precancerous vulvar conditions, and lichen sclerosus.
Other less common types of vulvar cancer include:
- Verrucous carcinoma: This is a slow-growing subtype of squamous cell carcinoma that has a wart-like appearance.
- Adenocarcinoma: Originating in the Bartholin’s glands or vulvar sweat glands, adenocarcinoma constitutes a small percentage of vulvar cancers. It is typically found on the sides of the vaginal opening.
- Melanoma: Accounting for about 2% to 4% of vulvar cancers, melanoma is a type of skin cancer usually found in sun-exposed areas of the body but can occasionally develop in non-sun-exposed regions. When it occurs in the vulva, it is most frequently found on the clitoris or labia minora. Women with melanoma elsewhere on their body face an increased risk of vulvar melanoma. Treatment for vulvar melanoma often follows approaches similar to those used for melanoma in other parts of the body.
- Sarcoma: Sarcoma involves tumors in the connective tissue beneath the skin.
It is essential to recognize these different types of vulvar cancer as they may necessitate distinct treatment strategies based on their specific characteristics.
What are the Symptoms of Vulvar Cancer?
The indications and symptoms of vulvar cancer can encompass the following:
- Persistent itch in the vulva
- Pain, soreness, or tenderness in the vulva
- Raised and thickened patches of skin that may appear red, white, or dark
- Presence of a lump or wart-like growth on the vulva
- Bleeding from the vulva or blood-stained vaginal discharge between periods
- Development of an open sore in the vulva
- Experiencing a burning pain during urination
- Noticeable changes in shape or color of a mole on the vulva
If any of these signs or symptoms persist or cause concern, it is essential to seek medical evaluation promptly for a thorough assessment and appropriate management.
What are the Causes of Vulvar Cancer?
The development of vulvar cancer cannot be predicted with certainty. While some women may experience these cancers without apparent high risk factors, certain elements may increase the likelihood of developing vaginal or vulvar cancer. These factors include:
- Increasing Age: The risk of vulvar cancer rises with age, with the average age at diagnosis being around 65 years.
- Exposure to Human Papillomavirus (HPV): HPV, a sexually transmitted infection, elevates the risk of various cancers, including vulvar and cervical cancers. Many sexually active individuals, especially the young, may come into contact with HPV, but in most cases, the infection clears up on its own. However, for some, it can cause cellular changes that increase the risk of cancer in the future.
- Smoking: For women with an HPV infection, smoking may hinder the body’s immune system from effectively clearing the HPV infection.
- Weakened Immune System: Individuals who take immune-suppressing medications (e.g., organ transplant recipients) or have conditions that weaken the immune system (e.g., human immunodeficiency virus, HIV) are at an increased risk of vulvar cancer.
- History of Precancerous Conditions of the Vulva: Vulvar intraepithelial neoplasia, a precancerous condition, raises the risk of vulvar cancer. Although most cases of vulvar intraepithelial neoplasia do not progress to cancer, a small number may develop into invasive vulvar cancer. As a precaution, doctors may recommend treatment to remove the abnormal cell area and conduct regular follow-up checks.
- Skin Condition Involving the Vulva: Lichen sclerosus is a condition that affects the vulvar skin, causing it to become thin and itchy, thereby increasing the risk of vulvar cancer.
Though these factors can contribute to an increased risk, it’s important to remember that not everyone with these risk factors will develop vulvar cancer, and some cases may occur without any identifiable risk factors. Regular check-ups and early detection remain essential for timely management and improved outcomes.
How Can I Lower My Chance of Getting Vulvar Cancer?
Various factors contribute to different types of cancer, including vulvar cancer. Researchers are actively investigating the causes of vulvar cancer and exploring preventive measures. While there is no guaranteed method to completely prevent vulvar cancer, certain steps can be taken to potentially reduce the risk. It is crucial to discuss your individual risk of cancer with your healthcare team for personalized information.
To aid in the detection of vulvar cancer, the doctor will review your family medical history, conduct a comprehensive physical examination, and perform a gynecologic exam focusing on the pelvis. During this exam, the doctor will carefully assess the vulva and perform checks on the uterus, vagina, cervix, and other reproductive organs for any unusual changes. Regular pelvic examinations are valuable in identifying cancer or precancerous conditions at an early stage.
Moreover, research has revealed specific factors that can potentially help in preventing vulvar cancer:
- Delaying first sexual intercourse until the late teens or older.
- Avoiding sexual intercourse with multiple partners.
- Avoiding sexual intercourse with individuals who have had numerous partners.
- Practicing safe sex, including condom use. Nevertheless, it is essential to acknowledge that condoms cannot provide complete protection against HPV. Abstinence from sexual intercourse remains the only method for full protection against HPV.
- Undergoing regular gynecologic examinations to detect and treat precancerous conditions.
- Quitting tobacco use for individuals who smoke.
By adopting these preventive measures and staying vigilant with regular check-ups, you can take proactive steps toward reducing the risk of vulvar cancer and promoting overall health. Remember to consult with your healthcare provider for personalized guidance and recommendations.
How is Vulvar Cancer Detected?
The diagnostic process for vulvar cancer involves various tests and procedures, including:
- Physical examination of the vulva: Your doctor will perform a thorough physical examination of your vulva to identify any abnormalities or concerning signs.
- Colposcopy examination: During a colposcopy, a special magnifying device is utilized to closely inspect the vulva for any abnormal areas. This enables a more detailed assessment of any suspicious regions.
- Biopsy: If an area of the vulva appears suspicious, a biopsy may be recommended to determine whether it is cancerous. During the biopsy procedure, the area is numbed with a local anesthetic, and a scalpel or other specialized cutting tool is used to remove a sample of the suspicious tissue for further testing.
These tests and procedures play a crucial role in diagnosing vulvar cancer accurately. If you experience any symptoms or have concerns about your vulvar health, it is essential to seek prompt medical evaluation to ensure timely diagnosis and appropriate management.
What are the Stages of Vulvar Cancer?
Stage groupings in cancer are determined based on the values of T (Tumor), N (Nodes), and M (Metastasis). These groupings provide an overall description of the extent of cancer in the body.
T = Tumor: This refers to the location and size of the primary tumor.
N = Nodes: Indicates whether the tumor has spread to nearby lymph nodes.
M = Metastasis: Determines whether cancer has spread to other parts of the body.
Each letter is accompanied by five numbered stages, ranging from 0 to 4, depending on the extent of cancer spread. Lower stage numbers indicate that the cancer cells closely resemble normal cells, making them more manageable and potentially curable. Conversely, higher stage numbers signify a deeper spread of the cancer, which may require more complex treatments and have a more challenging prognosis. Understanding the stage grouping is critical for determining the appropriate treatment plan and predicting the course of the disease.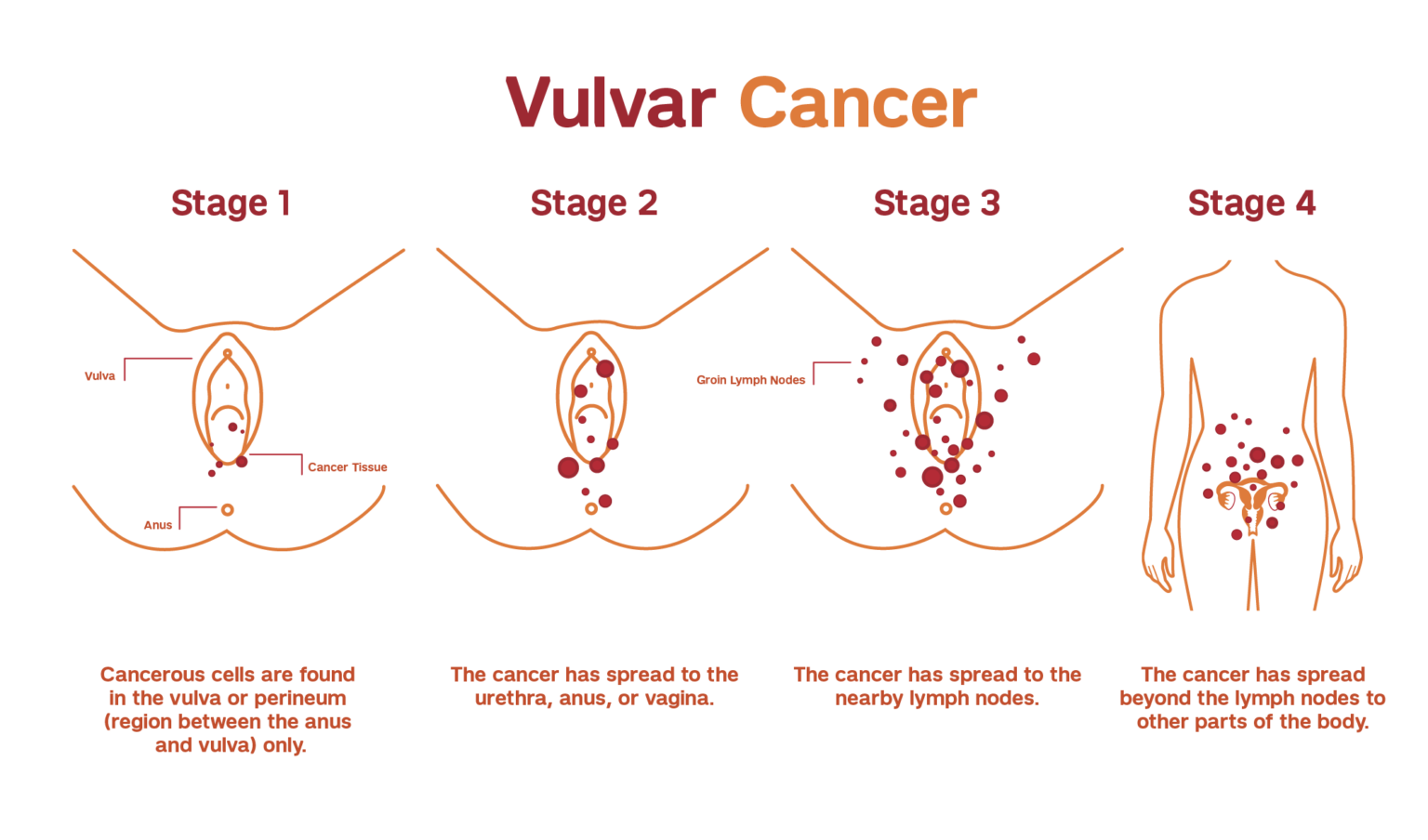
Stage groupings for invasive vulvar cancer are represented by Roman numerals, with values ranging from I (1) to IV (4). A higher stage number indicates a more advanced and extensive spread of the cancer.
The staging process for invasive vulvar cancer is determined by surgical findings and pathology. However, it’s important to note that stages for vulvar melanoma are distinct and not discussed in this context.
Stage I. The cancer is located either in the vulva or in the area between the opening of the rectum and the vagina (perineum), or it may involve both regions. At this stage, the cancer has not spread to nearby lymph nodes or other parts of the body. This stage is further divided into two substages:
Stage IA. The tumor size is limited to 2 centimeters (cm) or smaller, and its depth of growth into the vulvar tissue is no more than 1 millimeter (mm).
Stage IB. The tumor measures over 2 centimeters (cm) in size and/or has extended more than 1 millimeter (mm) beneath the surface of the vulvar skin.
- Stage II. The tumor can be of any size and has extended beyond the vulva, reaching nearby sites such as the urethra, lower vagina, or anus. However, it has not spread to lymph nodes or other distant parts of the body.
Stage III. The cancer is present in either the vulva, the perineum, or both. There is a possibility that it has spread to the urethra, lower vagina, or anus, but it has not extended to organs in distant parts of the body. This stage is further divided into three substages.:
Stage IIIA. The cancer has metastasized either to a single lymph node measuring at least 5 mm across, or to one or two lymph nodes that are less than 5 mm across.
Stage IIIB. The cancer has disseminated to three or more lymph nodes, each measuring no more than 5 mm across, or it has spread to two or more lymph nodes, each measuring more than 5 mm across.
Stage IIIC. The cancer has extended to adjacent lymph nodes, and in at least one of these nodes, the cancer is growing beyond its outer layer, a condition known as extracapsular spread.
Stage IV. This stage is divided into 2 substages:
The cancer is present in either the vulva, the perineum, or both. It is uncertain whether it has spread to the urethra, lower vagina, or anus. However, it has extended to nearby lymph nodes, which are adhering to deeper tissues or have developed ulcers.
The cancer has progressed beyond adjacent tissues and reached the upper part of the urethra, upper vagina, bladder, rectum, or pelvic bone. It is uncertain whether it has also spread to nearby lymph nodes.
What are the Treatments for Vulvar Cancer?
The treatment options for vulvar cancer are determined by factors such as the type, stage, and location of the cancer, as well as your overall health and personal preferences.
Surgery
Surgical procedures used to treat vulvar cancer include:
- Excision (Wide Local Excision or Radical Excision): The cancer and a small portion of surrounding healthy tissue are surgically removed to ensure complete elimination of cancerous cells.
- Vulvectomy (Partial or Radical): For larger cancers, surgery may involve the removal of part of the vulva (partial vulvectomy) or the entire vulva, including underlying tissue (radical vulvectomy). In some cases, radiation therapy and chemotherapy may be used before surgery to shrink the tumor, potentially allowing for a less extensive operation.
- Sentinel Node Biopsy: To assess the presence of cancer in the lymph nodes, a procedure called sentinel node biopsy is performed. It identifies the lymph nodes most likely to contain cancer, which can then be removed and examined. If cancer is not detected in these lymph nodes, the likelihood of it being present in other lymph nodes is low.
- Removal of Multiple Lymph Nodes: If cancer has spread to the lymph nodes, a significant number of lymph nodes may be removed to reduce the risk of cancer spreading to distant areas of the body.
Undergoing surgery involves potential complications, including infection and challenges related to healing around the incision site. Additionally, when lymph nodes are removed, there is a risk of developing lymphedema, a condition characterized by fluid retention and swelling in the legs.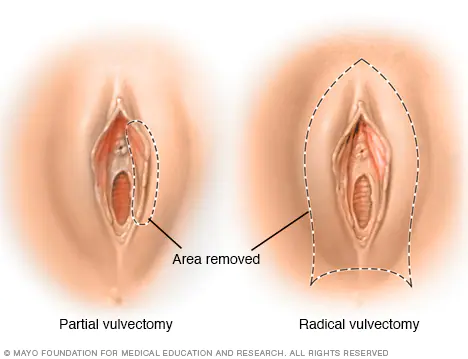
Radiation Therapy
Radiation therapy employs high-powered energy beams, such as X-rays and protons, to target and destroy cancer cells. In the context of vulvar cancer, radiation therapy is often delivered through a machine that moves around the body, precisely directing radiation to specific points on the skin (known as external beam radiation).
This treatment approach is sometimes used to reduce the size of large vulvar cancers, increasing the likelihood of a successful surgery. Combining radiation therapy with chemotherapy is also an option, as chemotherapy can render cancer cells more susceptible to the effects of radiation.
Furthermore, if cancer cells are detected in the lymph nodes, your doctor may recommend radiation therapy to the area surrounding the lymph nodes. This is intended to eliminate any remaining cancer cells after surgery. In certain cases, radiation therapy is combined with chemotherapy to maximize its effectiveness in these situations.
Chemotheraphy
Chemotherapy is a medical treatment that employs chemical substances to target and destroy cancer cells. Typically, these drugs are administered either through a vein in the arm or by mouth.
In cases of advanced vulvar cancer that has spread to distant areas of the body, chemotherapy may be considered as a treatment option.
Combining chemotherapy with radiation therapy is also utilized to reduce the size of large vulvar cancers, enhancing the chances of a successful surgical procedure. Additionally, when cancer has spread to the lymph nodes, combining chemotherapy with radiation therapy can be an effective approach in treatment.
Targeted Drug Theraphy
Targeted drug treatments are designed to specifically target and inhibit the abnormalities found within cancer cells. By blocking these specific abnormalities, targeted drug treatments can trigger the death of cancer cells.
For individuals with advanced vulvar cancer, targeted therapy may be considered as a potential treatment option.
Immunotherapy
Immunotherapy harnesses the power of your immune system to combat cancer. In some cases, cancer cells can evade detection by producing proteins that enable them to evade the immune system’s attack. Immunotherapy intervenes in this process, allowing the immune system to recognize and target cancer cells effectively.
For individuals with advanced vulvar cancer, immunotherapy could be considered as a potential treatment option.
NYGSE Approach
We recognize that receiving a cancer diagnosis can be an overwhelming and daunting experience. At NYGSE, our dedicated teams are centered around your well-being. Our skilled oncologists are committed to supporting you through this challenging journey, offering guidance and addressing any concerns you may have.
Rest assured that we are here for you, and our utmost priority is to cater to your individual needs, striving to surpass your expectations. If you or a loved one are experiencing symptoms that could be related to cancer, we urge you to contact us as soon as possible. Your health and care are of the utmost importance to us.
We provide specialized vulvar cancer treatment for patients in Babylon, Bay Shore, and surrounding Long Island communities.
Types of Gynecologic Cancer
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.
Have Questions About Your Surgery or Treatment?
Expert treatment. Compassionate care. Real results.
November 10, 2025by admin
Fallopian Tube Cancer
Understanding Fallopian Tube Cancer
Fallopian tube cancer is a rare but serious condition that originates in the narrow passage connecting the ovaries and uterus. Because its early symptoms often resemble other gynecologic conditions, it can be difficult to detect in its earliest stages. At New York Gynecology Surgery & Endometriosis (NYGSE), our specialists use advanced imaging, genetic insight, and minimally invasive surgical techniques to identify and treat fallopian tube cancers with precision. We’re committed to helping women receive an accurate diagnosis and the most effective, personalized treatment plan possible.
COMMON QUESTIONS ABOUT FALLOPIAN TUBE CANCER
What is Fallopian Tube Cancer?
Fallopian tube cancer, also referred to as tubal cancer, emerges within the fallopian tubes, which serve as the connecting pathway between the ovaries and the uterus. This type of cancer is exceptionally uncommon, accounting for only 1 to 2 percent of all gynecologic cancers. Globally, there have been reports of 1,500 to 2,000 cases of fallopian tube cancer. In the United States, approximately 300 to 400 women are diagnosed with this condition each year.
Interestingly, cancer more frequently originates from other parts of the body, like the ovaries or endometrium, and then spreads to the fallopian tubes rather than having its primary origin in the fallopian tubes themselves.
The typical age range of women affected by fallopian tube cancer is between 50 and 60, although it can develop at any age. Caucasians, particularly those who have had few or no children, are more prone to this type of cancer.
Due to its rarity, limited knowledge exists regarding the specific causes of fallopian tube cancer. However, researchers are exploring the potential role of genetics in its development. Some evidence suggests that women who have inherited the BRCA1 gene, which is associated with breast and ovarian cancer, may have an increased risk of developing fallopian tube cancer.
Recent findings have led doctors to consider that many high-grade serous type epithelial ovarian cancers, which are among the most common ovarian cancers, might actually initiate in the distal end of the fallopian tube, rather than on the surface of the ovary.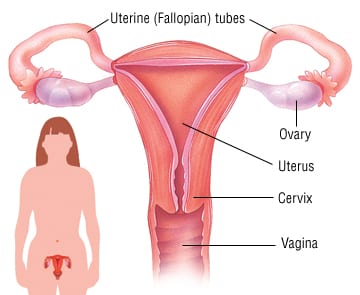
What are the Types of Fallopian Tube Cancer?
Fallopian tube cancers mainly consist of epithelial or surface carcinomas, which implies that they originate from the tissue lining or covering the fallopian tubes.
There are various types of fallopian tube cancers, including:
- Papillary serous adenocarcinomas: This type accounts for more than 95 percent of all fallopian tube cancers. It arises from the cells that line the fallopian tubes. As these cells undergo abnormal division and invade other organs or spread to different parts of the body, tumors can develop.
- Primary fallopian tube cancer: Primary fallopian tube cancer is an exceptionally rare form, making up about 1 percent of all gynecologic cancers.
- Sarcomas (leiomyosarcomas): In some cases, tumors called sarcomas (leiomyosarcomas) may originate from the smooth muscle within the fallopian tubes.
- Transitional cell carcinomas: Tumors can also form on the other cells that line the fallopian tubes, known as transitional cell carcinomas.
What are the Symptoms of Fallopian Tube Cancer?
Detecting fallopian tube cancer can be challenging as its symptoms often overlap with those of various common conditions experienced during menopause, which is a time when this type of cancer commonly occurs.
Symptoms may include:
- Abdominal swelling
- Abdominal and back pain
- Loss of appetite or feeling full quickly
- Frequent or urgent need to urinate, along with changes in toilet patterns, such as alterations in bowel habits
- Unexplained weight loss or gain
- Indigestion or heartburn
- Fatigue
- Watery discharge from the vagina.
If you experience any of these symptoms, it’s essential to consult your doctor. While these signs could be attributed to causes other than cancer, seeking medical advice is the only way to determine the underlying cause accurately.
What are the Causes of Fallopian Tube Cancer?
The specific cause of fallopian tube cancer remains unknown; however, certain factors are suspected to increase the risk, including: cost like 600
- Advancing age (most cases are diagnosed in women between 50 and 60 years old).
- Post-menopausal status.
- Nulliparity (having no children).
- Family history of ovarian or breast cancer, particularly among close relatives (mother, sister, daughter).
- Increased risk associated with inherited mutations in the BRCA gene, which are linked to higher incidences of ovarian and breast cancers.
- Never having breastfed a child.
- Never having used birth control pills.
- Presence of endometriosis, a benign (non-cancerous) condition that can elevate the risk of ovarian and fallopian tube cancers.
How Can I Lower My Chance of Getting Fallopian Tube Cancer?
Various factors contribute to different types of cancer, and researchers are actively investigating the causes and prevention of ovarian and fallopian tube cancer. While there is no definitive way to completely prevent these cancers, it may be possible to lower one’s risk. Consulting your healthcare team can provide valuable insights into your individual cancer risk.
Studies have indicated that certain factors may reduce the risk of developing ovarian and fallopian tube cancer:
- Taking birth control pills: Individuals who have used oral contraceptives for three or more years have shown a 30% to 50% lower likelihood of developing ovarian and fallopian tube cancer. This decreased risk might persist for up to 30 years after discontinuing the pills. Additionally, intrauterine devices (IUDs) have been associated with a reduced risk of ovarian cancer.
- Breastfeeding: Prolonged breastfeeding after childbirth is linked to a decreased risk of ovarian and fallopian tube cancer.
- Pregnancy: The number of full-term pregnancies a person has experienced is inversely related to their risk of ovarian and fallopian tube cancer.
- Surgical procedures: People who have undergone a hysterectomy or tubal ligation tend to have a lower risk of developing ovarian and fallopian tube cancer. A hysterectomy involves removing the uterus and sometimes the cervix. Tubal ligation is a surgical procedure where the fallopian tubes are tied or closed to prevent pregnancy. For individuals at high risk of ovarian and fallopian tube cancer, doctors might recommend bilateral salpingo-oophorectomy, which involves removing both ovaries and fallopian tubes. Some individuals choose to have their fallopian tubes removed during abdominal surgery for other purposes or during a caesarean section after completing their desired number of childbirths.
- High-risk genetic mutations: Individuals with genetic mutations like BRCA1, BRCA2, and genes associated with Lynch syndrome are advised to consider removing their ovaries and fallopian tubes after completing childbearing. This preventive measure can reduce the risk of ovarian and fallopian tube cancers by up to 96%. Furthermore, if the surgery is performed before natural menopause, there may be a 40% to 70% decrease in the risk of developing breast cancer, especially for individuals with BRCA2 mutations.
How is Fallopian Tube Cancer Detected?
Due to the rarity of fallopian tube cancer and its symptoms resembling other conditions, diagnosing it can be challenging. Sometimes, women only discover they have fallopian tube cancer when a tube is surgically removed during treatment for another health issue.
However, several tests can aid in definitively diagnosing the condition. Your doctor will begin by inquiring about any symptoms you may be experiencing, reviewing your medical history, and conducting a thorough physical examination. Additional tests that may be performed include:
- Pelvic Exam: This involves the examination of the uterus, vagina, ovaries, fallopian tubes, bladder, and rectum to detect any abnormalities in size or shape.
- CA125 Test: A blood test to measure CA125 levels, a tumor marker associated with gynecological diseases, including fallopian tube cancer. While approximately 85 percent of women with gynecological diseases have elevated CA125 levels, it’s crucial to note that increased CA125 levels may not necessarily indicate cancer. Levels can also rise during pregnancy, menstruation, and other non-cancerous gynecological diseases or cancers affecting different parts of the body.
- Computed Tomography (CT) Scan: This imaging test captures detailed pictures of the body’s internal areas. A computer, linked to an X-ray machine, generates these images. To enhance organ or tissue visibility, a special dye may be injected into a vein or swallowed.
- Ultrasound: Pelvic ultrasound uses high-frequency sound waves to create images of organs and systems within the body. These sound waves, inaudible to humans, produce a pattern of echoes called a sonogram, which can differentiate between healthy tissues, fluid-filled cysts, and tumors.
- PET (Positron Emission Tomography): PET scans involve the use of a radioactive sugar (glucose) to identify cancer cells. This test is sometimes employed to detect the spread of fallopian tube cancer.
These tests collectively aid in achieving an accurate diagnosis and better understanding the extent of fallopian tube cancer if present.
What are the Stages of Fallopian Tube Cancer?
The stages of fallopian tube cancer are determined by the extent of its spread, ranging from the earliest (Stage I) to the most advanced (Stage IV):
- Stage I: Cancer is confined to one or both fallopian tubes.
- Stage II: Cancer has extended to the uterus or nearby tissues within the pelvic region (which includes internal reproductive organs, bladder, and rectum), or it is localized on the peritoneum.
- Stage III: Cancer has progressed beyond the pelvic region and spread to lymph nodes and/or other abdominal areas (such as the surface of the liver or spleen).
- Stage IV: Cancer has metastasized to distant locations, such as the lungs.
What are the Treatments for Fallopian Tube Cancer?
Surgery plays a crucial role in the treatment of ovarian and fallopian tube cancers, and it is typically carried out by a gynecologic oncologist, a specialist in treating gynecologic cancers, including surgical procedures and chemotherapy (see “Chemotherapy” below).
As mentioned earlier in the Diagnosis section, surgery is often necessary to fully assess the extent of the disease and establish an accurate stage. Minimally invasive surgery is commonly employed to confirm the diagnosis and determine whether a debulking procedure (see below) should be performed immediately after diagnosis or after administering chemotherapy first. This step is essential because imaging tests may not always reveal the complete extent of the disease.
For patients with localized cancer in the ovary, a debulking procedure includes a staging process, involving the removal of various tissues, including lymph nodes, to determine if the cancer has spread. In advanced cases, the primary objective is to remove as much cancer as possible. This procedure has been shown to be most effective when combined with chemotherapy after the surgery.
There are several surgical options for ovarian and fallopian tube cancer, and the recommended surgeries depend on the tumor’s stage. In some cases, multiple procedures may be performed during the same surgery:
- Salpingo-oophorectomy: This surgery involves the removal of the ovaries and fallopian tubes. When both ovaries and both fallopian tubes are removed, it is referred to as bilateral salpingo-oophorectomy. For individuals with early-stage cancer who desire future pregnancy, it may be possible to remove only one ovary and one fallopian tube if the cancer is limited to one ovary. This type of surgery is known as unilateral salpingo-oophorectomy. For patients with a germ cell type of ovarian tumor, it is often sufficient to remove only the ovary containing the tumor, preserving the ability to conceive.
- Hysterectomy: This procedure involves the removal of the uterus and surrounding tissue if necessary. If only the uterus is removed, it is called a partial hysterectomy. A total hysterectomy includes the removal of both the uterus and the cervix.
- Lymphadenectomy/lymph node dissection: During this surgery, the surgeon may remove lymph nodes in the pelvic and paraortic regions.
- Omentectomy: This surgery aims to remove the thin tissue covering the stomach and intestines.
- Cytoreductive/debulking surgery: Used for advanced ovarian and fallopian tube cancers, the goal of this surgery is to remove as much tumor as safely possible. It may involve removing tissue from nearby organs, such as the spleen, liver, and parts of the small bowel or colon. This can alleviate symptoms caused by masses pressing on other organs and enhance the effectiveness of subsequent treatments, such as chemotherapy, to control any remaining disease. If the cancer has spread beyond the ovaries, fallopian tubes, or peritoneum, doctors may use neoadjuvant chemotherapy to shrink the tumor before cytoreductive or debulking surgery. Neoadjuvant chemotherapy involves 2 to 3 cycles of chemotherapy before the surgery to make the debulking procedure safer and more effective. Hyperthermic intraperitoneal chemotherapy (HIPEC), a newly described method, is being studied in clinical trials and is not yet the standard of care. Sometimes, chemotherapy may be administered during surgery.
It is advisable to have debulking surgery performed by a board-certified gynecologic oncologist if possible. Before undergoing surgery, discuss the risks and benefits of the procedure with your doctor. Inquire about the surgeon’s experience with debulking surgery and whether it will be conducted minimally invasively, through an open incision, or robotically. Make sure to explore the various surgical options with your doctor.
Therapies Using Medication
The treatment plan may involve medications aimed at destroying cancer cells. These medications can be administered through the bloodstream to target cancer cells throughout the body, a process known as systemic therapy. Alternatively, medication may be applied directly to the cancer or confined to a specific area of the body, which is referred to as local therapy.
A medical oncologist, a specialist in cancer treatment with medication, typically prescribes this form of treatment. Medications are often administered through an intravenous (IV) tube inserted into a vein using a needle or in the form of oral pills or capsules that are swallowed. When given intravenously, a port, a small plastic or metal disc placed under the skin before treatment begins, is often used to access the vein. For patients receiving oral medications, it’s essential to inquire about proper storage and handling guidelines from the healthcare team.
The types of medications used for ovarian, fallopian tube, and peritoneal cancer include:
- Chemotherapy
- Targeted therapy
- Immunotherapy
- Hormone therapy (in rare cases)
An individual may receive a single type of medication or a combination of medications simultaneously to treat their cancer. These medications may also be included as part of a comprehensive treatment plan that involves surgery and/or radiation therapy.
The medications used for cancer treatment are continually under evaluation. Discussing these medications with your doctor is crucial to understanding their purpose, potential side effects, and possible interactions with other medications. It’s essential to inform your doctor about any other prescriptions, over-the-counter medications, or supplements you may be taking. Certain herbs, supplements, and other drugs can interact with cancer medications, leading to unwanted side effects or reduced effectiveness. Utilizing searchable drug databases can help you gain more information about your prescriptions.
Radiation Therapy
Radiation therapy is not a primary treatment for ovarian or fallopian tube cancer. It may be used in select situations—such as early-stage clear cell ovarian cancer after chemotherapy, or for small, localized recurrences. It can also help manage symptoms or treat cancer that has spread.
Radiation therapy uses high-energy x-rays or particles to destroy cancer cells. Most patients receive external-beam radiation, delivered by a machine outside the body. Less commonly, internal radiation (brachytherapy) is used, in which a small radioactive source is placed near the tumor.
Proton therapy, a newer form of treatment, targets tumors more precisely by using protons instead of x-rays.
Typical side effects include fatigue, mild skin irritation, stomach upset, and loose stools, which usually resolve soon after treatment.
Radiation may also be part of care for recurrent or metastatic disease, often in combination with chemotherapy, targeted therapy, or immunotherapy to improve control and comfort. In advanced cases, palliative radiation can help relieve pain or other symptoms.
Because every case is unique, your treatment plan should be developed by a gynecologic oncologist in consultation with radiation and medical oncologists experienced in ovarian and fallopian tube cancers.
NYGSE Approach
We understand that a cancer diagnosis can be overwhelming and scary. Here at NYGSE, we build our teams around you. Our expert oncologists will help guide you through this difficult time, answering any questions you may have along the way. We are here for you and will do everything in our power to meet your specific needs and exceed your expectations.
If you or a loved one is experiencing symptoms that may be related to cancer, please call us as soon as possible.
We provide specialized fallopian tube cancer treatment for patients in Babylon, Bay Shore, and surrounding Long Island communities.
Types of Gynecologic Cancer
Pankaj Singhal, MD, MS, MHCM
With over 12 years of experience in both academic and private healthcare, Dr. Singhal has trained more than 45 gynecologic surgeons and fellows in minimally invasive and oncologic procedures. He has pioneered new surgical techniques for endometriosis and laparoscopic surgery, completing more than 5,700 robotic-assisted cases nationwide. Renowned for taking on the most complex cases other centers turn away, Dr. Singhal continues to advance the standard of women’s surgical care.